
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dayal Institute of Pharmaceutical Science, , Next to Indra canal Lucknow -226501, U.P. India.
The demand for effective and patient-friendly insulin administration systems has become increasingly important due to the rising incidence of diabetes mellitus. Even though subcutaneous insulin injection is still the recommended course of treatment, patients frequently experience poor compliance, pain, and diminished acceptance as a result of repeated injections. The unique physiological characteristics of the lungs, such as substantial vascularization, vast absorptive surface area, and quick systemic uptake, have drawn a lot of interest to pulmonary insulin delivery as a non-invasive option in recent years. The efficiency of inhaled insulin therapy has greatly increased thanks to technological developments in dry powder inhalers, aerosol formulations, and carrier-based systems. Multiple research studies have shown that inhaled insulin can improve patient convenience while providing quick glycemic control on track with injectable versions. However, its widespread clinical use is still restricted by issues such limited bioavailability, pulmonary deposition variability, formulation instability, and long-term pulmonary safety concerns. These restrictions might be addressed by new approaches involving formulations based on nanoparticles, efficient breathing devices, and enhanced particle engineering. The recent advancements, present difficulties, and potential future developments related to inhaled insulin delivery devices are outlined in this review.
Diabetes mellitus (DM) is a group of metabolic diseases distinguished by impaired protein, lipid, and carbohydrate metabolism as well as chronically elevated blood glucose (BG). DM may trigger acute complications including hyperosmolar hyperglycemic syndrome (HHS) and diabetic ketoacidosis (DKA) if it is not properly treated.
Microvascular, macrovascular, and neuropathic problems can result from long-term hyperglycemia. Conventional subcutaneous insulin delivery has a number of drawbacks despite its therapeutic efficacy, including as discomfort, needle anxiety, local tissue responses, and poor patient adherence over extended treatment. These disadvantages have prompted the creation of substitute non-invasive insulin delivery methods. Because the lungs allow for quick absorption and direct systemic availability of therapeutic drugs, pulmonary administration has emerged as one of the most promising techniques among those studied.
The pulmonary route's thin alveolar epithelium, vast capillary network, and comparatively modest enzymatic activity have drawn considerable amount of academic interest. Inhaled insulin therapy has advanced thanks to recent advancements in formulation development and inhalation technology.
1.1 Pathophysiology of Type-1 & Type-2 Diabetes Mellitus
In 5%–10% of instances, type 1 diabetes usually occurs by autoimmune destruction of pancreatic β-cells, which eventually ends in a complete lack of insulin. Although it can happen at any age, it typically manifests in children and teenagers. It is thought that exposure to an unclear environmental trigger in a genetically predisposed person causes the illness. Macrophages and T lymphocytes with autoantibodies to β-cell antigens (such as insulin and islet cell antibodies) mediate the autoimmune process, Because β-cells are destroyed in type 1 diabetes, amylin, a hormone derived from pancreatic β-cells with insulin, is also deficient. Amylin causes central feelings of fullness, delays stomach emptying, and inhibits incorrect glucagon secretion. Following the initial diagnosis, there may be a brief period of remission known as the "honeymoon" phase, during which insulin dosages can be lowered or stopped until ongoing β-cell breakdown demands lifetime insulin replacement medication.
Type 2 diabetes (90%–95% of cases) Decreased insulin secretion: β-cell failure is gradual, and β-cell bulk and function are decreased. Diminished incretin effect: Following a meal, the gut incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) are typically released and increase insulin secretion. Insulin resistance or lower amounts of the incretin hormones cause patients with type 2 diabetes to have a diminished incretin impact. This is characterized by increased lipolysis and the synthesis of free fatty acids, impaired skeletal muscle absorption of glucose, and excessive hepatic glucose production. Excess glucagon secretion: GLP-1 resistance/deficiency and insulin resistance/deficiency, which directly suppress glucagon, prevent type 2 DM patients from suppressing glucagon in response to meals. Renal increase of sodium-glucose cotransporter-2 (SGLT-2): This causes the proximal renal tubular cells to reabsorb more glucose, which exacerbates hyperglycemia.
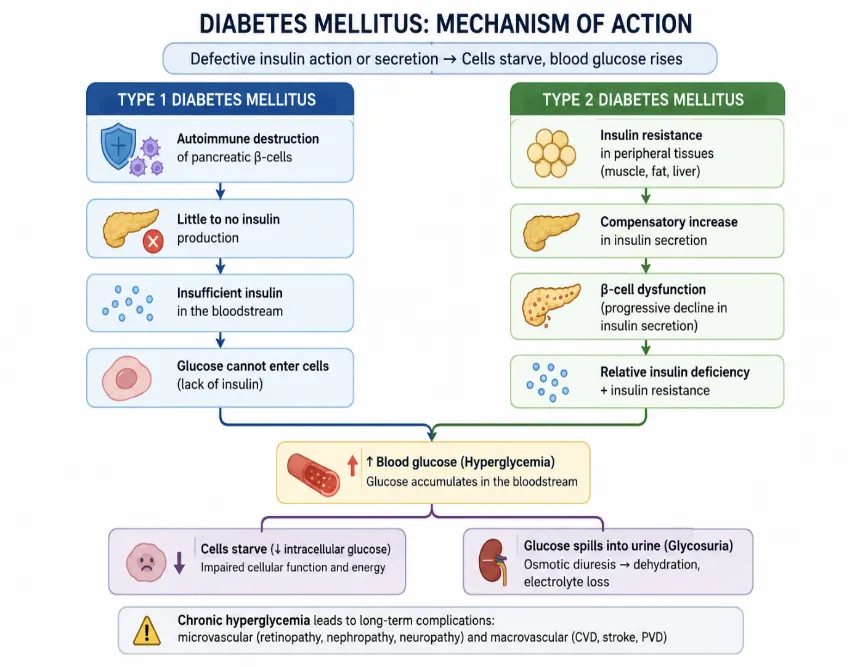
Figure-1: Diabetes Mellitus- Mechanism of Action
2. Diabetes Mellitus and Need for Alternative Insulin Delivery
Many diabetic patients still find insulin injection therapy to be challenging, especially if they need several daily doses. Frequent injections may have a negative impact on glucose control and reduce treatment adherence. Additionally, lipodystrophy, psychological resistance to long-term insulin administration, and local discomfort are frequently linked to conventional injectable therapy. As a result, numerous studies have been conducted on alternative insulin delivery methods, including oral, nasal, buccal, transdermal, and pulmonary systems. In addition to the lungs' immense surface area and extremely permeable epithelial membrane, pulmonary administration has shown significant promise among these methods for the systemic absorption of proteins and peptides.
In contrast to oral treatment, pulmonary transport avoids hepatic first-pass metabolism and gastrointestinal degradation, increasing the likelihood of quick therapeutic action. Because inhaled insulin devices are non-invasive and simple to administer, they may also increase patient acceptance.
3. How to Work Pulmonary Delivery of Insulin
Because of their structural and physiological features, the lungs are considered to be an effective route for systemic medication administration. Because of the alveolar region's large surface area and high vascularization, inhaled chemicals can enter the bloodstream quickly. Particle size, airflow dynamics, inhalation method, and formulation qualities all play a major role in successful pulmonary delivery.
For extensive lung deposition, particles with aerodynamic sizes between 1 and 5 µm are typically thought to be ideal. While very small particles may be expelled prior to deposition, larger particles typically build up in the upper respiratory tract. Thus, preserving suitable particle properties is crucial for increasing treatment efficacy. In addition to their ease and stability, dry powder inhalers have emerged as one of the most extensively studied inhaled insulin delivery devices.
The turbulence produced by airflow during inhalation helps disperse powder and promotes deposition in the lower respiratory tract. However, dosage administration and absorption may be impacted by patient differences in lung health and aspiratory flow rate.
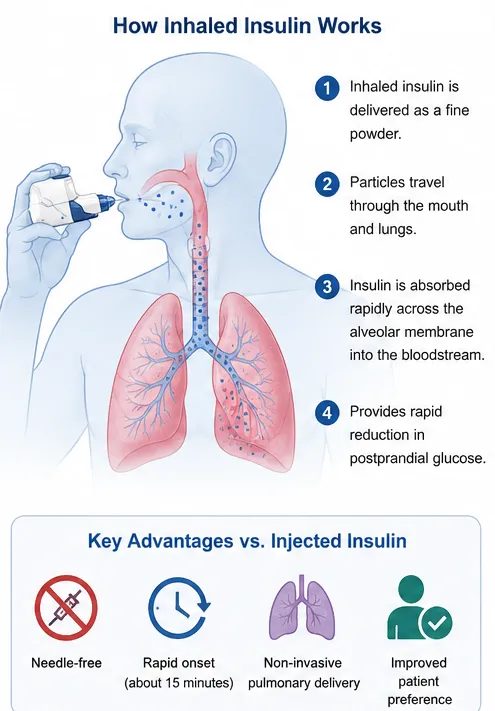
Figure-2: How to work Pulmonary Delivery of Insulin
4. Formulation and Delivery Systems
To improve systemic bioavailability and pulmonary insulin delivery, a number of formulation techniques have been developed. Because dry powder formulations are more stable, portable, and convenient to store than liquid solutions, they are still widely used. For effective pulmonary administration, nebulized and aerosolized insulin formulations have also been investigated.
Research on inhaled insulin has benefited greatly from recent developments in nanotechnology. Liposomes, polymeric nanoparticles, and solid lipid nanoparticles are examples of nanocarrier systems that have demonstrated promise for enhancing lung retention and absorption while shielding insulin from deterioration.
Additionally, these carriers may limit medication release and improve formulation stability.
Delivery efficiency is significantly influenced by inhalation devices in addition to formulation techniques. Modern inhalers are made to maximize lung deposition, aerosol production, and airflow resistance. Dosage uniformity and treatment results may be further enhanced by technological advancements involving computationally built devices and smart inhalers.
5. Clinical Applications and Marketed Products
For the treatment of type 1 and type 2 diabetes mellitus, inhaled insulin has been thoroughly investigated. According to clinical research, pulmonary insulin administration has a quicker onset of action and can provide glucose control on par with traditional subcutaneous therapy.
The first inhaled insulin medication made available for therapeutic use was called Exuberant. Despite showing therapeutic efficacy, its high cost, large inhalation devices, and poor patient acceptance prevented it from becoming commercially successful. Later, Afrezza was created as a fast-acting inhaled insulin with better pharmacokinetic performance and device design.
According to clinical research, a lot of people prefer inhaled insulin because it doesn't cause the discomfort that comes with repeated injections. Additionally, improved postprandial glucose regulation is supported by rapid pulmonary absorption.
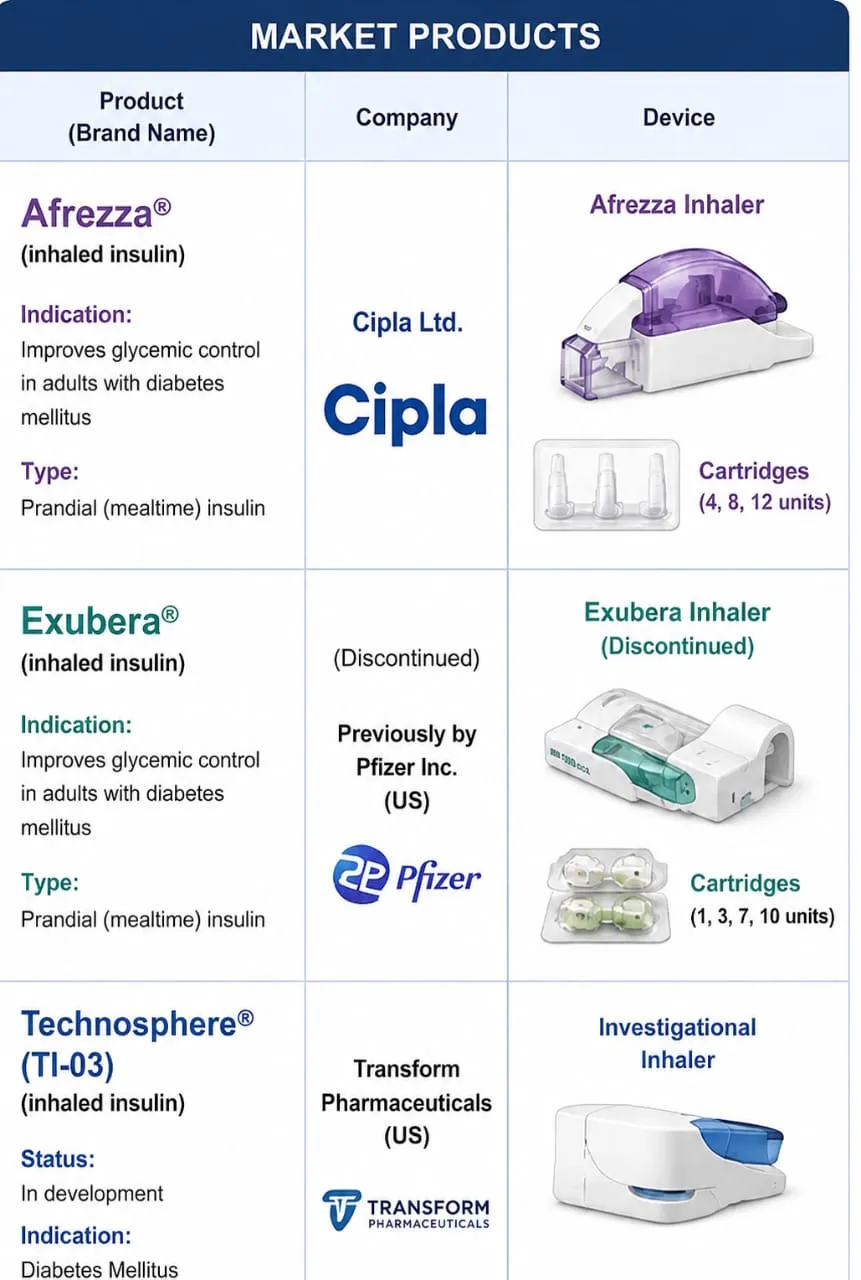

Figure-3: Clinical Application & Market Product of Inhaled Insulin
6. Advantages of Inhaled Insulin
Pulmonary insulin delivery offers several advantages over traditional injectable therapy. Because inhaled insulin is non-invasive, it is more convenient for patients and may encourage them to start insulin treatment. When compared to standard subcutaneous insulin, rapid absorption via the alveolar membrane also helps to accelerate the onset of action.
Additional advantages include
• Enhanced adherence to treatment
• Reduction of pain from needles
• Less anxiety associated with injections
• Easy administration
• A higher level of patient satisfaction
• Possible enhancement of postprandial glucose regulation
Because of these advantages, inhaled insulin is a desirable option for managing diabetes over the long run.
7. Pulmonary Challenges and Limitations
The clinical success of inhaled insulin systems continues to be challenged by a number of issues, despite significant advancements. The comparatively low pulmonary bioavailability brought on by incomplete lung deposition, particle aggregation, mucociliary clearance, and macrophage uptake is one of the main issues.
Pulmonary safety over the long run is still a major concern. Cough, throat discomfort, and slight changes in pulmonary function have been described by some individuals undergoing inhaled insulin therapy. Furthermore, respiratory conditions such asthma, smoking-related lung disease, and chronic obstructive pulmonary disease may have a substantial impact on the absorption of insulin and the consistency of treatment.
Additional obstacles to widespread clinical application include formulation instability, moisture sensitivity, dosage variability, and high manufacturing costs. Maintaining formulation stability during storage and achieving repeatable deep lung deposition remain significant scientific concerns.
8. Recent Advances and Future Perspectives
The therapeutic potential of inhaled insulin systems has been enhanced by recent advancements in nanomedicine and inhalation technology. Formulations with improved aerosolization and greater pulmonary deposition can now be produced thanks to advanced particle engineering processes.
In order to improve insulin stability and extend medication retention in the lungs, nanotechnology-based carriers such as liposomes, polymeric nanoparticles, and microspheres are presently being studied. In a similar vein, contemporary dry powder inhalers with enhanced dispersion mechanisms and optimized airflow resistance may improve the effectiveness of dose administration.
It will be expected that future studies would concentrate on enhancing pulmonary safety, boosting bioavailability, reducing dose variability, and creating inhalation devices that are easy for patients to use. Smart inhaler integration with digital monitoring systems may enhance medication adherence and provide more individualized diabetic care.
CONCLUSION
A possible non-invasive method for managing diabetes that may increase patient acceptability of insulin therapy is inhaled insulin administration. Compared to traditional injectable formulations, the pulmonary route offers quick absorption, easy administration, and a quicker commencement of therapeutic activity. The efficiency of pulmonary insulin delivery has increased due to notable advancements in aerosol technologies, nanocarrier systems, and dry powder inhalers. However, issues with dosage variability, limited bioavailability, formulation stability, and pulmonary toxicity still prevent widespread clinical usage. Future success and wider adoption of inhaled insulin therapy may be influenced by ongoing developments in formulation science and inhalation technology.
Acknowledgement
The authors are thankful to Dr. Amit Kumar Singh Director, Dayal groups of Institution Lucknow for providing library facility to carry out the literature survey.
REFERENCES





Pooja Singh, Mohd Zafar Khan, Abdul Hameed, Dewashish Jaiswal, Bushra Shaukat Review Article: Insulin Inhaler– Current Advances, Challenges, and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 7008-7014, https://doi.org/10.5281/zenodo.20960158
 10.5281/zenodo.20960158
10.5281/zenodo.20960158