
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Principal K. M. Kundnani College of Pharmacy, Cuffe Parade, Mumbai – 400 005
Arthritis is one of the most prevalent chronic musculoskeletal conditions, affecting millions worldwide and significantly reducing quality of life. Characterized by joint inflammation, stiffness, swelling, and progressive disability, arthritis primarily exists in two major forms: osteoarthritis (OA), a degenerative joint disease, and rheumatoid arthritis (RA), an autoimmune systemic disorder. Current management relies on synthetic drugs such as non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and disease-modifying antirheumatic drugs (DMARDs). While these agents provide symptomatic relief, their long-term use is often associated with gastrointestinal, renal, hepatic, and immunosuppressive complications. Consequently, there is a rising demand for safer and more sustainable alternatives. Phytomedicine, rooted in traditional medical systems such as Ayurveda, Siddha, and Traditional Chinese Medicine, has emerged as a promising complementary approach. Herbal drugs such as:Curcuma longa (curcumin), Boswelliaserrata (shallaki), Withaniasomnifera (ashwagandha),Tinospora cordifolia (guduchi), Commiphora mukul (guggul) possesses anti-inflammatory, antioxidant, and immunomodulatory properties. Modern drug delivery innovations, including phytosomes, nanoemulsions, emulgels, and nanocarriers, have further enhanced their therapeutic potential. This review provides a comprehensive overview of the mechanistic basis of arthritis, conventional therapies, limitations of synthetic drugs, rationale for herbal alternatives, clinical evidence, and future prospects for phytomedicine in arthritis management
Arthritis is a broad term encompassing over 100 rheumatic diseases and conditions that affect joints, surrounding tissues, and connective structures. It represents one of the leading causes of disability worldwide, with an estimated global prevalence of more than 350 million individuals. Osteoarthritis (OA) and rheumatoid arthritis (RA) are the most common and debilitating forms [1].
Osteoarthritis (OA): A degenerative joint disorder characterized by the progressive breakdown of articular cartilage, subchondral bone remodeling, and limited joint mobility. It is strongly associated with aging, obesity, and repetitive mechanical stress.
Rheumatoid arthritis (RA): A chronic autoimmune inflammatory disease leading to synovial membrane inflammation, pannus formation, cartilage erosion, and joint deformity. Unlike OA, RA is systemic and often accompanied by extra-articular manifestations such as cardiovascular and pulmonary complications [2].
The global burden of arthritis continues to rise due to increased life expectancy, sedentary lifestyles, and obesity prevalence. The World Health Organization (WHO) recognizes musculoskeletal conditions, including arthritis, as major contributors to disability-adjusted life years (DALYs). The limitations of conventional synthetic drugs, coupled with the long duration of arthritis treatment, have prompted growing interest in phytomedicine [3]. Herbal medicines not only offer symptomatic relief but also exert disease-modifying actions with minimal toxicity, making them attractive candidates for long-term management.
FIG. 1 FIG. 2
FIG. 3 FIG. 4
Etiological factors:
Genetic predisposition: HLA-DR4 and HLA-DRB1 alleles increase susceptibility to RA.
Age: Degenerative changes accumulate with aging, making OA more common in older adults.
Sex: RA is more prevalent in women; gout is more common in men.
Autoimmune dysregulation: Aberrant immune activation triggers chronic inflammation in RA and systemic lupus erythematosus (SLE).
Metabolic disorders: Uric acid crystal deposition (gout) and calcium pyrophosphate deposition (pseudogout).
Infection: Septic arthritis may arise from bacterial invasion.
Mechanical stress and trauma: Obesity, repetitive joint use, and prior injury accelerate OA progression.
FIG. 5 FIG. 6
2. PATHOGENESIS:
• Genetic and environmental factors such as smoking, infections, and hormonal influences initiate immune dysregulation.
• Antigen-presenting cells including macrophages and dendritic cells activate T-lymphocytes.
• Activated T-cells release pro-inflammatory cytokines such as IL-1, IL-6, TNF-α, and IFN-γ.
• Cytokine release stimulates B-cell proliferation and activation [4].
• B-cells differentiate into plasma cells that produce autoantibodies including rheumatoid factor (RF) and anti-citrullinated peptide antibodies (ACPAs).
• Immune complex deposition within the synovial membrane activates the complement system.
• Activated macrophages release inflammatory mediators such as TNF-α and IL-1, promoting synovial hyperplasia and pannus formation.
• Matrix metalloproteinases (MMPs) degrade cartilage and contribute to progressive joint destruction.
• • The inflammatory cascade ultimately leads to joint swelling, stiffness, pain, deformity, and progressive disability.
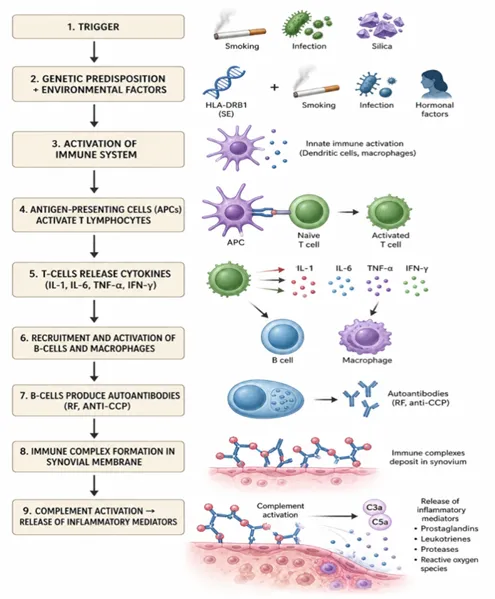
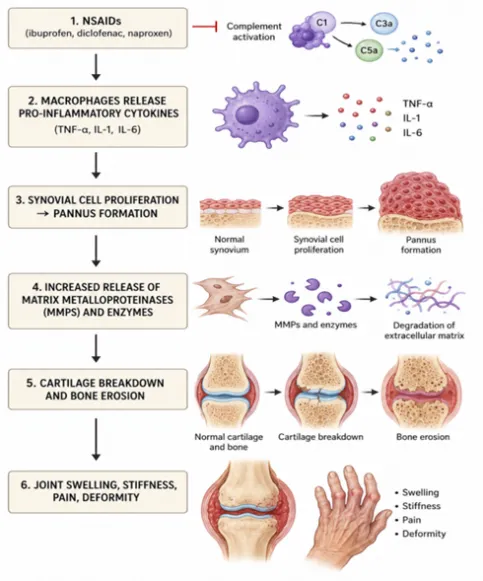
FIG 7 FIG 8
3. CONVENTIONAL THERAPIES FOR ARTHRITIS
1.Classes of Drugs
Provide symptomatic relief by inhibiting cyclooxygenase enzymes, reducing prostaglandin synthesis [5,6].
Corticosteroids
(e.g., prednisone, dexamethasone):
Potent anti-inflammatory and immunosuppressive agents used in acute exacerbations.
DMARDs
(e.g., methotrexate, leflunomide, sulfasalazine, hydroxychloroquine):
Slow disease progression and reduce joint damage.
Biologic agents
(e.g., anti-TNF-α, IL-6 inhibitors, JAK inhibitors): Target specific cytokines or signaling pathways.
2.Limitations
Gastrointestinal bleeding and ulcers (NSAIDs).
Immunosuppression, osteoporosis, metabolic changes (corticosteroids).
Hepatotoxicity, bone marrow suppression (DMARDs).
High cost and infection risk (biologics) [7].
Hence, there is a need for safer alternatives, especially for long-term therapy.
TABLE NO. 1: Drugs used in Arthritis Management
|
Class |
Action |
Drugs |
|
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) |
Reduce pain, inflammation, and stiffness by inhibiting cyclooxygenase (COX) enzymes and prostaglandin synthesis |
Ibuprofen, Naproxen, Diclofenac, Indomethacin |
|
Glucocorticoids (Corticosteroids) |
Potent anti-inflammatory and immunosuppressive agents used for rapid symptom relief |
Prednisolone, Hydrocortisone, Dexamethasone, Methylprednisolone |
|
Disease-Modifying Antirheumatic Drugs (DMARDs) |
Alter the progression of disease, suppress immune-mediated inflammation, and prevent joint damage |
Methotrexate, Leflunomide, Sulfasalazine, Hydroxychloroquine[8,9] |
Rationale for Herbal/Phytomedicine Use
1.Global Perspective
WHO estimates 80% of the world’s population relies on traditional medicine for primary healthcare. In Europe and North America, herbal supplements such as turmeric, boswellia, ginger, and willow bark are widely used as complementary therapies.
Countries like India, China, and Japan integrate herbal medicine into modern rheumatology.
2.AYUSH Perspective
The Ministry of AYUSH actively promotes herbal remedies for arthritis.
Research councils like CCRAS (Central Council for Research in Ayurvedic Sciences) conduct clinical trials on herbs such as Boswellia serrata, Tinospora cordifolia, and Withaniasomnifera. Initiatives like AYUSH e-pharma strengthen herbal drug distribution and awareness [10].
4. HERBAL DRUGS IN ARTHRITIS MANAGEMENT
1. Curcuma longa (Turmeric, Curcumin)
Mechanism: Inhibits NF-κB, COX-2, and LOX pathways; reduces oxidative stress.
Clinical evidence: Curcumin combined with diclofenac improved knee OA outcomes with fewer side effects.
2. Boswellia serrata (Shallaki)
Active compound: Boswellic acids inhibit 5-lipoxygenase.
Benefits: Reduces cartilage degradation, joint swelling, and pain.
3. Withaniasomnifera (Ashwagandha)
Acts as an adaptogen and immunomodulator.
Reduces pro-inflammatory cytokines and oxidative stress.
4. Tinospora cordifolia (Guduchi)
Enhances immune regulation and reduces "Ama" (toxins) in Ayurvedic concept. Shown to inhibit autoimmune arthritis in preclinical studies [11].
5.Commiphora mukul (Guggul)
Contains guggulsterones; exhibits lipid-lowering and anti-inflammatory activity.
6. Zingiber officinale (Ginger)
Active compounds (gingerols, shogaols) reduce TNF-α and IL-1β expression. Provides analgesic and anti-inflammatory effects [12].
FIG. 9 FIG. 10
FIG. 11
TABLE NO. 2 TABLE NO. 3
Advances in Herbal Drug Delivery
1. Emulgels
Combination of emulsion and gel systems.
Enhance penetration, provide non-greasy texture. Example: Boswellia + Ginger herbal emulgel.
2. Nanoparticles
Increase solubility and absorption of poorly soluble phytoconstituents like curcumin. Allow targeted delivery to inflamed joints.
3. Phytosomes
Complex of herbal extract and phospholipids.
Example: Curcumin phytosomes with higher oral bioavailability [13].
4. Transdermal Patches
Provide controlled release of herbal actives. Improve patient compliance.
5.Nanoemulsions and Liposomes
Enhance stability and absorption of herbal drugs.
Protect thermolabile compounds from degradation
TABLE NO. 4 : Benefits of Herbal Drugs over Conventional Drugs
|
Parameter |
Herbal Drugs |
Conventional Drugs |
|
Mechanism of Action |
Multi-targeted action including anti-inflammatory, antioxidant, immunomodulatory, and cartilage-protective effects |
Usually acts through a single or specific pathway such as COX inhibition, immunosuppression, or TNF/IL blockade |
|
Safety Profile |
Generally associated with fewer gastrointestinal, renal, and hepatic adverse effects when standardized and used appropriately; considered safer for long-term use |
Long-term use may lead to ulcers, gastrointestinal bleeding, hepatotoxicity, nephrotoxicity, osteoporosis, and other adverse effects |
|
Tolerance |
Better tolerated during chronic administration (e.g., formulations containing turmeric, Boswellia, or Ashwagandha) |
Often poorly tolerated during prolonged therapy due to cumulative adverse effects [14] |
|
Holistic Balance |
Supports overall immunity, vitality, metabolism, and associated comorbid conditions along with disease management |
Primarily focuses on symptomatic or disease-specific treatment; may produce systemic side effects |
|
Drug–Drug Interaction |
Comparatively fewer interactions when standardized formulations are used under supervision |
Higher potential for interactions, especially with DMARDs, corticosteroids, NSAIDs, and biologics |
|
Cost Effectiveness |
Relatively affordable and accessible, particularly in resource-limited settings |
Expensive, especially biologics and long-term DMARD therapy |
|
Patient Acceptability |
High patient acceptability due to natural origin and perceived safety |
Moderate acceptability because of concerns regarding adverse effects, dependency, and long-term toxicity [15] |
Role of Standardization &Quality Control
• Lack of uniformity in herbal drug preparations may result in variable therapeutic efficacy and inconsistent clinical outcomes.
• Need for standardization of herbal formulations to ensure quality, safety, and reproducibility.
• Identification and authentication of raw materials are essential to avoid adulteration and contamination.
• Use of standard phytochemical markers such as curcumin and boswellic acids helps maintain consistency in herbal products.
• Adherence to pharmacopeial standards including the Ayurvedic Pharmacopoeia of India (API), World Health Organization guidelines, and Ministry of AYUSH regulations is necessary for quality assurance [16].
• Application of advanced quality control techniques such as HPTLC, HPLC, GC-MS, and DNA fingerprinting improves standardization and authentication.
• Proper standardization ensures product safety, batch-to-batch reproducibility, therapeutic reliability, and enhanced patient trust.
5. CLINICAL EVIDENCE
Case Study A: Curcumin Phytosome (Meriva®) in Osteoarthritis
Design: Prospective randomized clinical trial.
Dose: 500 mg tablets twice daily (1 g/day delivering ~200 mg curcuminoids).
TABLE NO. 5
|
Observation (Median Decrease After Eight Months) |
Treatment Group |
Control Group |
|
Decrease in Gastrointestinal Complications |
63.4% |
8% |
|
Decrease in Management Costs |
63.5% |
3.7% |
Results:
Improved WOMAC and Karnofsky scores.
Reduced use of NSAIDs.
Lowered CRP and ESR levels. No major adverse events.
Conclusion: Curcumin phytosome provides effective and safe OA management.
Case Study B: Boswellia serrata Nano-Emulgel
Design: Preclinical + in vitro diffusion + in vivo animal studies.
Formulation: 5% Boswellia serrata extract in carbopol-based nanoemulgel.
FIG. 12 FIG. 13
Results:
~98.5% in-vitro permeation in 5 h.
Superior anti-inflammatory and analgesic effect.
Comparable or better efficacy than diclofenac in some assays [17].
Conclusion: Nano-emulgel offers enhanced local delivery and therapeutic effect
6. FUTURE PROSPECTS:
• Integration of herbal medicines with nanotechnology to enhance solubility, bioavailability, targeted delivery, and therapeutic efficacy.
• Development of novel nanoformulations such as liposomes, phytosomes, polymeric nanoparticles, and nanoemulsions for herbal drugs.
• Need for more randomized controlled clinical trials to establish scientific evidence, safety, and global acceptance of herbal therapies.
• Advancement of personalized phytomedicine approaches based on genetic, metabolic, and disease-specific patient profiles.
• Encouragement of public–private partnerships to promote translational research and commercialization of evidence-based herbal products.
• Strengthening regulatory frameworks and international standardization guidelines for herbal medicines.
• Application of artificial intelligence and machine learning in herbal drug discovery, formulation optimization, and prediction of therapeutic outcomes.
• Increased focus on sustainable sourcing, cultivation, and conservation of medicinal plants for long-term healthcare applications [18,19].
CONCLUSION
Both synthetic and herbal medicines have roles in arthritis therapy. However, the chronic nature of arthritis necessitates safer long-term strategies. Herbal medicines, supported by traditional wisdom and modern clinical validation, provide effective symptom relief and disease modification. Novel delivery systems such as phytosomes and nanoemulgels further enhance their therapeutic profile. Bridging traditional knowledge with scientific rigor can revolutionize arthritis management and improve patient quality of life.
CONFLICT OF INTEREST:The authors have no conflicts of interest.
REFERENCES

Ashish Manwani, Savi Nilawar, Amit Pawar, Pranchi Shethia, Nikhil Rajnani, Nalini Kurup Targeting Arthritis Through Phytomedicine: Mechanistic Understanding and Clinical Evidence, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4705-4713, https://doi.org/10.5281/zenodo.20748817
 10.5281/zenodo.20748817
10.5281/zenodo.20748817