
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Rajarambapu College of Pharmacy, Kasegaon, Walwa, 415404, Sangli, Maharashtra, India.
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by the loss of dopaminergic neurons in the substantia nigra and accumulation of ?-synuclein-containing Lewy bodies. It is the second most common neurodegenerative disorder, primarily affecting individuals above 65 years of age. Clinically, PD presents with motor symptoms such as tremor, rigidity, bradykinesia, and postural instability, along with non-motor complications. The etiology of PD is multifactorial, involving genetic and environmental factors, with key genes including SNCA, LRRK2, GBA, and MAPT contributing to disease progression. Current treatment strategies, such as L-DOPA therapy, pharmacological agents, cell therapy, and gene therapy, mainly provide symptomatic relief without halting disease progression. Recent advancements in genome editing, particularly CRISPR-Cas9 technology, have opened new avenues for understanding and treating PD. This system enables precise modification of target genes through DNA cleavage and repair mechanisms, including non-homologous end joining and homology-directed repair. CRISPR-Cas9 has shown potential in correcting genetic mutations, developing disease models, and advancing gene-based therapies. However, challenges such as off-target effects, delivery limitations, and ethical concerns hinder its clinical application. Overall, CRISPR-Cas9 represents a promising tool for future disease-modifying therapies in Parkinson’s disease.
Parkinson disease (PD) which people refer to as Idiopathic parkinsonism or primary parkinsonism or hypokinetic rigid syndrome or paralysis agitans stands as the second most common progressive neurodegenerative disorder which impacts 2% to 3% of people who reach 65 years of age. The disease demonstrates its neuropathological main feature through the degeneration process which destroys dopaminergic neurons in the substantia nigra and the subsequent intracellular buildup of alpha-synuclein (α-synuclein) material which forms Lewy body structures[1].The loss of nigrostriatal dopaminergic innervation in PD leads to neurodegeneration which affects both the dopaminergic neurons in the nigral area and cells in different parts of the neural system. PD demonstrates widespread pathology which results in highly variable manifestations but its diagnosis requires a dependable testing method that scientists have not developed yet. Doctors use clinical symptoms for diagnosis because patients must display two out of four specific clinical symptoms which include resting tremor and bradykinesia and rigidity and postural instability for them to qualify as having the condition[2]. Research has advanced understanding of Parkinson's disease epidemiology and disease causes yet scientists still do not know which factors trigger the disease. Clinical diagnostic criteria have developed in recent years to enhance diagnostic accuracy through their implementation. The condition remains difficult to diagnose especially during its initial stage when symptoms resemble those of multiple neurodegenerative diseases. Medical experts need to identify the early disease stages because research shows that most future disease-modifying therapies will be effective at this point. The medical field needs improved systems to classify Parkinson's disease into distinct subtypes based on patient symptoms and disease progression and its biological functions to create more effective individualized treatment methods[3].
Parkinson's disease (PD) pathological characteristics stem from the accumulation of misfolded a-synuclein in Lewy bodies (LBs) which are intracellular inclusions and the destruction of dopaminergic neurons in the substantia nigra (SN) pars compacta (SNpc). The initial diagnosis of patients demonstrates that they have already lost most of their dopaminergic neurons from the SNpc while neurodegeneration has spread to different regions of the central nervous system[4].
Researchers have identified 20 genes that contain monogenic mutations which lead to the development of Parkinson's disease. The research conducted by Zhang et al. discovered that human astrocytes show increased expression of certain monogenic mutations when they compared their transcriptome with that of neurons[5].
1. SNCA:
Scientists discovered α-synuclein protein aggregates as the main component of Lewy bodies which serve as the primary pathological hallmark of Parkinson's disease after they identified SNCA mutations as the cause of a rare monogenic form of Parkinson's disease. The discovery established a link between the development of monogenic and genetically complex forms of Parkinson's disease. The SNCA gene shows two risk factors for Parkinson's disease since its rare mutations and common genetic variations both function as disease risk factors. The REP1 polymorphism in the gene's promoter region showed a link to idiopathic Parkinson's disease which revealed that the SNCA locus contained genetic risk factors for the disease[6].
2. LRK:
The LRRK2 gene mutations account for 5-13% of all familial PD cases and 1-5% of all sporadic PD cases. The seven missense LRRK2 mutations which scientists identified as pathogenic include R1441G R1441C R1441H Y1699C G2019S R1628P G2385R I2020T because they exist in various functional domains of LRRK2. PARK-LRRK2 represents an individual case of Parkinson disease which shows no symptoms but carries a simplex genetic pattern. People with PARK-LRRK2 experience slower motor progression together with longer survival times compared to others[8].
3. GBA:
The GBA gene is located on chromosome 1 (1q21) and is made up of 11 exons. The gene encodes the lysosomal hydrolase enzyme glucocerebrosidase which is also known as GCase. GCase functions to cleave glycosphingolipids (GSLs) GlcCer and GlcSph into glucose and ceramide, and glucose and sphingosine, respectively. Different mutations in the GBA gene cause varying levels of GCase activity reduction because some mutations lead to complete enzyme activity loss while other mutations permit limited enzyme function. GCase activity shows specific reduction in human brains from GBA-PD patients, with the most severe decline found in the SNpc region[9].
4. MAPT:
The microtubule-associated protein tau (MAPT) exists as a phosphorylated protein which shows its primary location in the brain, where it functions to stabilize the neuronal cytoskeleton and support axonal transport activities. The discovery of dominantly inherited MAPT mutations established the first connection between tau protein dysfunction and neurodegenerative diseases, which include frontotemporal dementia and parkinsonism that occurs because of chromosome 17 mutations. The MAPT mutation spectrum includes clinical overlaps between FTD-parkinsonism and FTD-ALS as its constituent phenotypes. The mutations on MAPT gene cause the dysfunction of tau protein determining its accumulation in neurofibrillary tangles. Recent data show that patients who experience parkinsonism plus Parkinson disease (PD) frequently develop tau protein aggregation together with α-synuclein aggregation, which indicates that both proteins work together to drive the neurodegenerative process. The sporadic description of PD-ALS clinical complex, known as Brait–Fahn–Schwarz disease[11].
Doctors use clinical features of patients to diagnose Parkinson's disease because there are no effective lab tests for the disease. Doctors have worked hard to find the cause of Parkinson's disease but its origins remain unknown which prevents them from developing effective treatments for the condition[12].
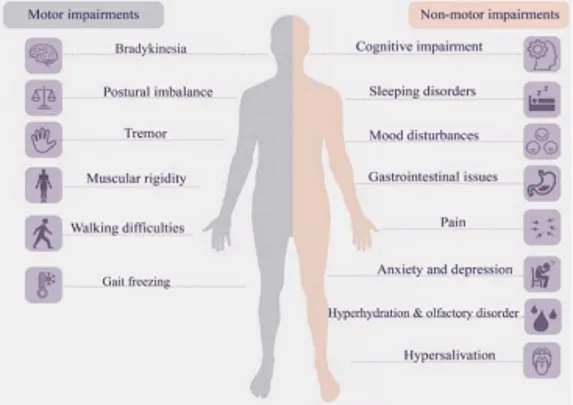
Fig 1; Clinical manifestations of PD
1. Pharmacological Treatments
The most frequently prescribed medications for cognitive impairment treatment are acetylcholinesterase inhibitors which include Donepezil and Galantamine and Rivastigmine [83]. Patients with Parkinson's disease who suffer from depression typically receive serotonin/norepinephrine reuptake inhibitors (SNRIs) treatment which includes Duloxetine and Desvenlafaxin and Milnacipran and venlafaxine. The available treatment options include benzodiazepines (e.g., Alprazolam and Clonazepam and Diazepam and Lorazepam) and selective serotonin reuptake inhibitors (SSRI) (e.g., Fluoxetine and Sertraline) and tricylic compounds (e.g., Amitrytiline and Imipramine and Nortriptyline) and additional anxiolytics (e.g., Buspirone and Propanolol and Quetiapine and Trazodone)[13].
2. L Dopa :
The first drug development attempts used l-dopa as the only treatment before researchers began testing the dopamine reuptake inhibitor and N-methyl-d-aspartate antagonist amantadine. The medical field started using ergot-based treatments which were later followed by non-ergot dopamine agonists and drugs that blocked dopa decarboxylase and monoamine oxidase B and catechol-O-methyltransferase enzymes. Scientists continue to debate l-dopa use because its treatment causes motor fluctuations and faster aging and there are worries about l-dopa's potential neurotoxic effects[14].
3. Cell therapies :
Scientists have studied cell-based methods which either restore dopamine-producing neurons or protect those neurons as potential treatments for Parkinson's disease since the disease was discovered. Clinical trials of cell-therapy for PD showed mixed results despite showing promising results in preclinical testing because researchers had not yet produced a complete review of the test results[15].
4. Gene therapy :
A) Researchers work on developing new treatments which will change the course of diseases through their research on gene therapy methods. The clinical trials use recombinant adeno-associated virus type 2 (rAAV2) and lentivirus vectors to investigate three main treatment methods which include increasing dopamine production through neurotransmitter synthesis and modifying neuronal characteristics and providing neuroprotection[16].
B) We have developed a gene therapy which delivers a working GBA1 gene to the central nervous system for patients who have Parkinson's disease and GBA mutations. Our investigational drug, called PR001, represents the first clinic-staged experimental gene therapy for these patients. We selected adeno-associated virus serotype 9 (AAV9) as our vector to deliver a codon-optimized plasmid which contains the wild-type human GBA1 gene[17].
The introduction of flexible genome-editing technologies during the last few years enables researchers to perform rapid and cost-effective genome editing work across multiple cell types and organisms. The core technologies now most commonly used to facilitate genome editing, shown in, are (1) clustered regularly interspaced short palindromic repeats (CRISPR)-CRISPR-associated protein 9 (Cas9), (2) transcription activator-like effector nucleases (TALENs), (3) zinc-finger nucleases (ZFNs), and (4) homing endonucleases or meganucleases[18].The CRISPR-Cas9 system comprises two fundamental components: the Cas9 protein and the guide RNA (gRNA). Cas9 operates as a molecular scissor, which uses gRNA to identify specific DNA locations for cutting. Scientists have adapted this molecular system, which originally emerged from bacterial immune defenses, for genome editing in multiple species, including humans because of its straightforward operational design and versatile capabilities. CRISPR-Cas9 operates as a powerful genome editing tool because the Cas9 protein and gRNA function together to create specific DNA sequence changes. The technology shows great potential to advance genetic research and create new therapeutic solutions[19].The gene editing process of the CRISPR/Cas9 system proceeds through three essential steps which include the three steps of recognition, cutting and repair. The target sequence is recognized by sgRNA through its 5'-crRNA which binds to the base pairs of the target gene, thereby directing the Cas9 nuclease to the designated target sequence. The Cas9 protein makes a DNA cut at 3 bp upstream of the PAM sequence after the RNA-DNA hybrid exists. The cell completes double-strand break repair through two processes which include non-homologous end joining (NHEJ) and homologous recombination (HDR). NHEJ serves as the primary DNA recovery pathway for cells which handles DNA breakages by directly connecting fractured DNA ends without needing a repair template. The process introduces insertions or deletions (indels) into the DNA sequence which results in gene mutations or gene inactivation[ 20].
The method enables scientists to delete or insert or change genes with exceptional accuracy, which establishes CRISPR-Cas9 as a powerful genetic research tool that has potential therapeutic uses. The new technology enables more researchers and institutions to perform advanced genetic modifications because it costs less than previous gene-editing methods, which has created more possibilities for innovation and discovery in fields such as agriculture and medicine and biotechnology[21].
(a) Identification phase: 1987–1993
The identification of the alkaline phosphatase isozyme conversion gene in Escherichia coli led to the first discovery of five direct repeats which contained 24 nucleotide repetitive sequences associated with the CRISPR-Cas system in 1987[22].
(b) Structural and functional characterization phase: 1993–2011.[22]
The CRISPR array is often preceded by an AT-rich leader sequence of up to 500 base pairs (bp).CRISPR loci exist in genomes which contain between one and 20 CRISPR loci that can extend from a few to several hundred repeat-spacer pairs. Chloroflexus sp. holds the current record for CRISPR with its 374 repeats and spacers. Researchers have identified 12 main CRISPR types based on similarities in the repeat sequences[23].
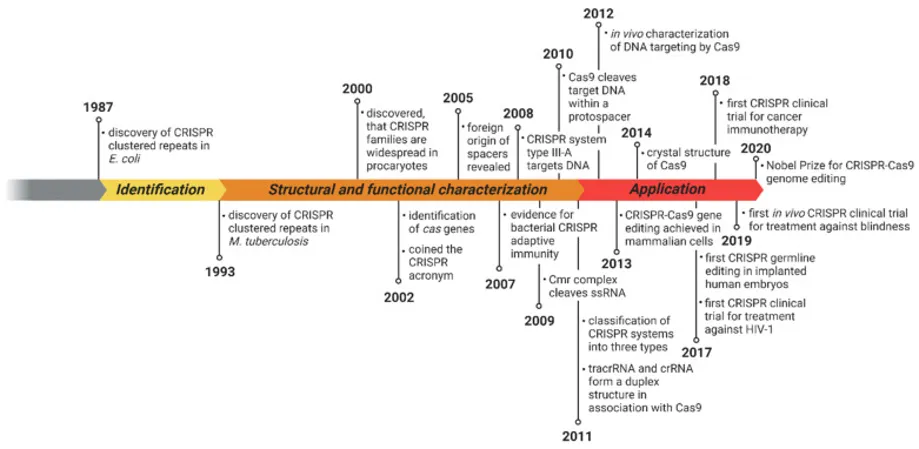
Fig 2: Timeline of the Clustered Regularly Interspaced Palindromic Repeats (CRISPR)–Cas system with important milestones[22].
S. pyogenes Cas9 (hereafter referred to as SpyCas9) is a large (1,368-amino-acid) multidomain and multifunctional DNA endonuclease. The enzyme cuts double-stranded DNA at a location 3 base pairs before the protospacer adjacent motif through its two nuclease domains which include an HNH-like domain that cuts the DNA sequence matching the guide RNA and an RuvC-like domain that cuts the DNA sequence opposite the matching strand. Cas9 serves as an essential element of CRISPR interference while it supports the development of crRNA and the collection of new spacer sequences[24].
Scientists developed the CRISPR system by creating an array which contains foreign DNA segments that they call spacers and which they positioned between segments of repeated DNA. The spacers function as genetic material which comes from previous plasmid or viral infections in the organism. Gene editing tools which include Cas nucleases see multiple improvements through new designs that enhance both target range and editing accuracy and editing efficiency (Koonin, 2019). CRISPR systems use Cas proteins for interference functions and these proteins also help create crRNAs in some systems which use CRISPR effector complexes. Cas proteins exist in different types which include effector proteins and adaptive proteins. The two adaptive Cas proteins Cas1 and Cas2 work together to develop new spacers which they create from incoming foreign DNA. The proteins Cas9 Cas12 and Cas13 function as effector Cas proteins which identify and cut specific target sequences[25].
The CRISPR/Cas-9 genome editing mechanism operates through three fundamental stages which include recognition and cleavage and repair. The sgRNA that was created by the researchers commands Cas-9 to identify the specific target sequence in the gene of interest through its 5ʹcrRNA complementary base pair component. The Cas-9 protein remains inactive in the absence of sgRNA. The Cas-9 nuclease creates double-stranded breaks (DSBs) at a location which is positioned 3 base pairs upstream of the PAM sequence. The PAM sequence functions as a short conserved DNA sequence which has a length of 2 to 5 base pairs and appears downstream of the cut site with its actual size varying according to the specific bacterial species. [26] The PAM interaction establishes PAM binding specificity through its interaction with target sequences. The HNH and RuvC domains function as nucleases to execute their target sequence cutting operation. The absence of gRNA prevents the Cas9 protein from entering its active state. The engineered gRNA forms a T-shape involved in 1 tetra-loop and 3 stem-loops. The gRNA contains a 5′ end programming which allows it to bind with the target sequence' complementary sequence [27].
After the Cas9 protein creates a double-stranded DNA break, the cellular DNA repair mechanisms are activated to repair the resulting DNA damage. The two primary repair pathways are:
The most frequently used repair system operates by restoring broken DNA segments through its rapid ability to reconnect their ends. The repair process of the system creates errors which lead to the formation of small DNA insertions or deletions that occur at the broken DNA connection point. The presence of these indel mutations in the gene sequence leads to functional disruption of genes which makes NHEJ suitable for conducting gene knockout studies[28].
DSB NHEJ → Insertions/Deletions
The CRISPR-Cas9 system operates as a precise genome editing method by using a donor template for double-strand break (DSB) repairs which it performs with exceptional precision. The system enables precise genetic modifications through HDR which allows for exact gene insertions deletions and substitutions while NHEJ introduces mistakes during the process[29].
DSB + Donor Template HDR→ Precise Gene Correction
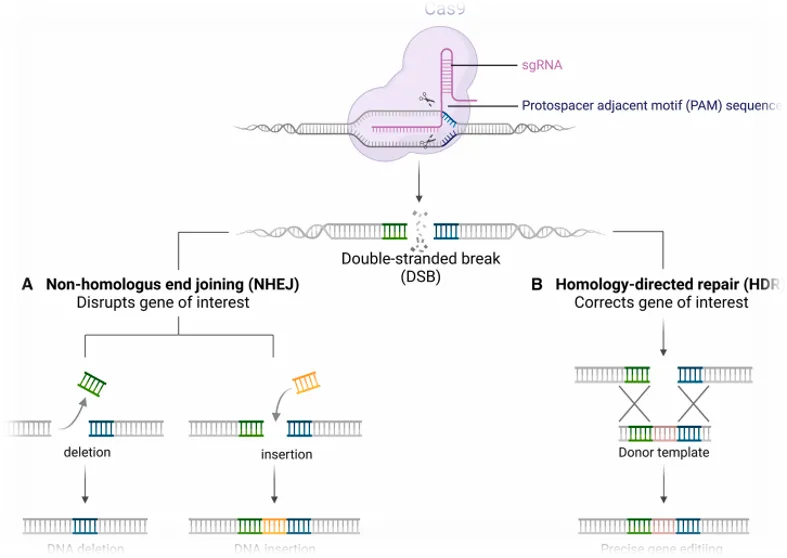
Fig no.3 Mechanism of CRISPR CAS9[29]
Scientists use iPSCs to convert patient cells into stem cells which they modify for research on genetic variations between cells from identical twin studies. FACS-assisted CRISPR/Cas-9 editing created isogenic lines from PD patients with the SNCA mutation who showed early mitochondrial impairment through their decreased capabilities to produce maximum respiration and basal respiration and ATP synthesis. The most frequent genetic basis for PD results from LRRK2 mutations. A study performed a cytogenetic analysis of a G2019S mutation in LRRK2, which the researchers corrected through CRISPR system, the team succeeded in developing a footprint-free LRRK2-G2019S isogenic human iPSC line through their application of CRISPR system and piggyBac technologies, the results indicate that human CRISPR-based mutation corrections could enable permanent resolution of Parkinson's disease genetic mutations through this method[30].
1. Researchers use CRISPR-Cas9 technology to investigate multiple genetic disorders that include hemophilia, Duchenne muscular dystrophy α1-antitrypsin deficiency hearing loss and hematopoietic diseases[31].
2. CRISPR-Cas9 technology holds significant promise for revolutionizing agriculture through its ability to create exact and effective genetic changes in both crops and livestock breeding programs[32].
3. The application of CRISPR-Cas9 technology in environmental sciences creates potential pathways for solving environmental problems and protecting natural resources and implementing environmentally sustainable methods[32].
4. The genome editing tool CRISPR-Cas9 shows high research laboratory usage because it enables scientists to study oncogene functions in cancer cells. The process of using CRSIPR-Cas9 to change cancer genes offers new possibilities for developing cancer treatments[33].
5. In vivo delivery:
Researchers have used adeno-associated virus (AAV) as a viral vector to enable effective CRISPR-Cas9 delivery in their studies. The Cas9 gene has a size range of 4 to 7 kilobases while adeno-associated viruses can only carry DNA up to their maximum limit of 4.7 kilobases. The most effective method for delivering nucleases into living organisms involves using non-viral systems that transmit direct mRNA or protein molecules[33].
6. In Immunotherapy:
The early experimental work together with the beginning stages of clinical trials demonstrate that CRISPR-engineered cell therapies achieve successful treatment results. The B cell cancer treatment method which uses chimeric antigen receptor (CAR) T cells to target CD19 has successfully achieved extended remission for patients with treatment-resistant SLE and rheumatoid arthritis by eliminating autoreactive B cells and restoring immune system balance[34].
7. Neurological Disorders:
Researchers can use CRISPR to stop Huntington's disease progression by disabling the HTT gene which causes the neurodegenerative disease. Researchers can use CRISPR to slow down ALS progression by targeting the SOD1 and C9orf72 genetic mutations which cause the disease.
Scientists can use CRISPR to change the genes associated with Parkinson's and Alzheimer's disease which will enable them to create new treatment options even though they must conduct more research[35].
8. Environmental Conservation:
The control of invasive species occurs through CRISPR-based gene drives which create inheritance bias for particular traits to manage invasive species populations. The preservation of biodiversity occurs through CRISPR technology which enables endangered species rescue by two methods disease resistance enhancement and genetic diversity increase for vulnerable populations[35].
9. NHEJ gene knockouts
Scientists use CRISPR/Cas9 technology to create gene knockouts in organisms. This method lets researchers study how single or multiple target genes function. The targeted genes include enzyme genes and microRNAs. Researchers achieve this study by using gene mutation techniques[36].
10. Health Research:
The first clinical applications of CRISPR technology will occur through somatic cell therapies which use CRISPR for laboratory-based procedures because human germline cell editing remains banned due to ethical concerns and because gene therapy regulations still require establishment. The primary applications of CRISPR technology involve treating genetic disorders through direct treatments of monogenic disorders and using CRISPR to combat oncotic cells and viral infections[37].
The off-target problem of CRISPR-Cas9 systems creates a second obstacle because it causes unexpected biological changes that result in detrimental effects. The probability of off-target effects rises when there are over three PAM and sgRNA mismatches which can cause both genetic mutations and immune system reactions[38].
CRISPR technology suffers from problems that limit its operational efficiency. NHEJ outperforms HDR in flexibility because it provides better capabilities for various applications. Nanoparticles function as tools that boost the effectiveness of HDR. Certain genetic disorders require extensive genetic modifications that go beyond simple gene deletion. The team needs to test sgRNAs with Cas9 to determine their effectiveness[38].
The Adeno-Associated Viruses AAV vector system offers a potential delivery method for CRISPR/Cas9 systems but faces challenges because of its small packaging capacity and restricted target range. The researchers developed two methods to solve the problem because they needed to deliver the Cas9 protein which they had separated into two AAV vectors[39].
The potential of gene editing technologies, like CRISPR/Cas9, raises serious ethical and safety concerns. The technology's uses in molecular biology research, which include developing advanced police dogs and creation of crops with pest resistance, establish a framework for evaluating ethical and moral and safety challenges. Human germline alteration creates two main concerns because it can endanger human safety and dignity while also enabling potential genocide activities[39].
The revolutionary CRISPR-Cas9 genome editing technology holds the potential to transform human treatments for genetic disease. The system enables precise genomic alteration through three different genetic modification techniques which include insertion, knockout and fixed-point mutation. The range of CRISPR-Cas9 applications keeps expanding because of its ongoing technological improvements. The CRISPR-Cas9 tool empowers researchers to establish disease research mode while they identify pathogenic gene and study the function of target gene as well as its regulatory elements. The clinical use of CRISPR-Cas9 technology has created outstanding therapeutic possibilities because it can treat disorders caused by genetic mutations and numerous phase I clinical trials have been conducted. The field of CRISPR-based therapeutics advancement requires development of new Cas9 control techniques and scientists are working on new editor systems which include base and prime editors. Translational dCas9-based technologies have developed into a rising field because they enable researchers to control therapeutic target dosing and timing without creating DSBs, which solves existing problems with Cas9 usage[41].
REFERENCES

Prajakta Jadhav, Vaishnavi Khadang, Pranali Sakate, Saloni Itkarkar, Shantanu Bele, Vaishnavi Kumbhar, Shreya Patil, The Emerging Role of CRISPR-Cas9 in Parkinson's Disease Research and Treatment, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3786-3798. https://doi.org/10.5281/zenodo.20711128
 10.5281/zenodo.20711128
10.5281/zenodo.20711128