
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, S.V. U College of Pharmaceutical Sciences, Sri Venkateswara University, Tirupati, India
Wound healing is a dynamic and multi-stage biological process that involves the restoration of damaged tissues and protect the wound site from microbial infection. Conventional topical formulations such as creams, gels, and ointments are widely used; however, their therapeutic effectiveness is often limited because of poor skin penetration and inadequate drug retention. To overcome these limitations, advanced drug delivery systems have been developed. Transfersomes are a novel class of highly flexible vesicular carriers designed to improve transdermal drug delivery. Due to their ultra-deformable and elastic nature, these vesicles can pass through narrow skin pores and deliver both hydrophilic and lipophilic drugs into deeper layers of the skin. Since their development, transfersomes have gained significant attention for delivering a wide range of therapeutic agents, including anti-inflammatory drugs, antibiotics, proteins, and herbal compounds. These systems offer several advantages such as enhanced drug permeability, improved bioavailability, targeted delivery and reduced systemic side effects, thereby increasing patient compliance. Despite challenges related to stability and large-scale production, recent advancements such as transethosomes and hybrid vesicular carriers have shown promising improvements. Overall, transfersomes represent a promising and effective approach for enhancing wound healing by ensuring better drug delivery and localized therapeutic action.
Wound healing begins immediately after skin injury and involves a series of biological events that help in tissue repair and protection against infection. Various topical products such as creams, ointments and dressings are commonly used in treatment. However, these formulations mainly act on the surface and may not effectively deliver drugs into deeper layers of the skin, which can limit their overall effectiveness.
Nanocarriers are crucial for wound healing because they increase the bioavailability of drugs and have been demonstrated to improve drug delivery into the skin by altering pharmacokinetics and biodistribution. Penetration enhancer containing vesicles (PEVs), ethosomes, liposomes, niosomes, and transfersomes are vesicular systems that have been demonstrated to enhance the therapeutic activity of drugs used for wound healing. Because of their flexible form and enhanced surface hydrophilicity, transfersomes, which use hydration gradients as a driving force to carry the molecules into and across the skin. Hence they play a crucial role in enhancing transdermal drug transport.
Their ability to carry such a diverse range of substances makes them a useful tool in contemporary medicine for improving drug delivery and efficacy.[1]
1. WOUND HEALING
1.1 Importance of wound healing
Wound healing is important for restoring normal skin function and preventing infection. Skin function and preventing infection. It involves different biological components working together to repair the damaged area. Both local factors such as infection, temperature, and oxygen supply and systemic factors like overall health condition can influence the healing process. [2,3]
1.2 Physiology of Wound healing
Wound healing is a well organized process that occurs in response to tissue injury. After injury, platelets quickly accumulate at the site and form a clot to stop bleeding. At the same time, they release growth factors that help in attracting cells required for repair. Over time, new tissue forms and replaces the damaged area.
Depending on the condition, wounds may heal either by regeneration or scar formation. In some situations, excessive tissue formation can lead to abnormal scars such as keloids or hypertrophic scars. [4-7]
1.3 Types of Wound healing
Depending on how long they last and how they heal, wounds are usually classified as acute wounds and chronic wounds [8]. By the proper care, Acute wounds caused by corrosive chemicals, radiation, mechanical trauma, heat, or electrical shock, usually heal quickly. However, chronic wounds do not heal as quickly as acute wounds. Chronic wounds heal in accordance with the various steps and time period that define the typical wound-healing process, and they are associated with certain disorders, such as diabetes mellitus and factors such as moisture imbalance, necrotic tissue accumulation and bacterial load significantly delay chronic wound healing.
Furthermore, there is a very high risk that chronic wounds may reoccur unless the underlying cause of the sickness is treated [9]. In reality, chronic wounds may never heal at all or take years to recover. Therefore, it is essential to resolve the stage and get rid of these inhibiting influences. Wounds can also be classified into three groups based on their depth: (1) superficial wounds, which cause some epidermis to be lost; (2) partial-thickness wounds, which affect the epidermis and deeper dermal layers; and (3) full-thickness wounds, which rupture deeper tissue and subcutaneous fat [10].
1.4 Phases of Wound healing
Wound healing occurs in four stages: a) Hemostasis, b) Inflammation, c) Proliferation and d) Maturation. During hemostasis, blood clotting takes place to stop bleeding. The inflammatory phase helps remove the bacteria and damaged tissue. In the proliferation stage, new tissue and blood vessels are formed. Finally, during maturation, the regenerated tissue gradually becomes stronger and structurally organized. Both local and systemic factors can influence the speed and effectiveness of this process [11].
1.4.1 Hemostasis Phase
Hemostasis, the initial phase of healing, begins as soon as an injury develops in order to prevent blood loss and restrict the growth of germs [12]. Vascular constriction, platelet aggregation, and the development of a fibrin clot due to the activation of the thrombin enzyme are characteristics of this phase. This process aids in the formation of a solid clot to stop bleeding by facilitating platelet clumping. At this stage, platelets are activated and aggregate when they come into touch with collagen [13]. Furthermore, they release a number of growth factors (Table 1) such as transforming growth factor-β (TGF-β), insulin-like growth factor-1, platelet-derived growth factor (PDGF), and epidermal growth factor (EGF) that cause inflammation at the site of damage [12, 13, 14,15].
1.4.2 Inflammation/ Defensive Phase
The defensive/inflammatory phase, which occurs concurrently with homeostasis, it phase helps to eliminate microbial contamination, remove debris, and essentially prepare the wound bed for the formation of new tissues [12]. During this phase White blood cells, mainly neutrophils, macrophages, and lymphocytes, release a range of proinflammatory cytokines, cationic peptides, proteases, reactive oxygen species, and growth factors that aid in wound cleaning. Growth factors such as TGF-β, recombinant human Granulocyte macrophage-colony Stimulating Factor (GM-CSF), platelet-derived growth factor PDGF, fibroblast growth factor, basic fibroblast growth factor (BFGF), and EGF are essential for cell-to-cell communication, fibroblast, keratinocyte and angiogenesis stimulation, and immune cell attraction into the wound to eliminate bacteria, remove debris, and repair damaged tissues [12, 13]. Unused cells go through apoptosis when their role is terminated, which results in a decrease in their quantity. After that, waste is removed by specialized cells known as macrophages [17]. In order to recover the devitalized tissues and efferocytosis, these macrophages create growth factors and proteins that attract immune cells to wound. A prolonged inflammatory phase may result in cell destruction and disrupt extracellular remodelling composition, which delays epithelization [14, 15, 16]. Where efferocytosis is the removal of apoptotic neutrophils before they undergo secondary necrosis by macrophages to limit tissue damage and aid in its recovery. This stage is frequently marked by discomfort, heat, erythema, and edema.
Table.1 Growth factors and role [17]
|
Growth factors |
Role of growth factors in wound healing |
|
Epidermal growth factor EGF |
By stimulating fibroblast proliferation, discrimination, keratinocytes, and transmigration, they hasten epidermal regeneration. |
|
Basic fibroblast growth factor BFGF |
By encouraging the growth of fibroblasts, keratinocytes, and re-epithelialization, they increase extracellular deposition and collagenase synthesis. |
|
Granulocyte macrophage-colony Stimulating Factor GM-CSF |
By stimulating the proliferation and differentiation of macrophages, keratinocytes, endothelial cells, and eosinophils, they aid in the constriction of wounds and encourage the local recruitment of inflammatory cells. |
|
Platelet-derived growth factor PDGF |
By encouraging the proliferation of neutrophils, macrophages, and fibroblasts, they improve the structural integrity of vasculature, re-epithelialization, and matrix deposition. |
|
Transforming growth factor-β TGF-β |
By stimulating the proliferation and remodeling of macrophages, keratinocytes, lymphocytes, and fibroblasts, they facilitate the development of granulation tissue, matrix formation, and re-epithelialization. |
1.4.3 Proliferation Phase
Granulation, contraction, and re-epithelialization occurs in this phase [18]. The proliferative phase [19], which attempts to cover the wound with new tissues, begins after the lesion has been removed. Three distinct steps define this phase: 1) The wound is filled with granulation tissues; 2) The wound borders shrink; and 3) Re-epithelialization covers the wound [19]. During the initial phase (filling the wound), fibroblasts produce collagen, hyaluronan, fibronectin, glycosaminoglycan, and proteoglycan, while epithelial cells begin to replace dead cells. During this phase, glossy, deep red granulation tissue fills the wound bed with connective tissue and new blood vessels are created (angiogenesis). The movement of dermal and epidermal cells causes the wound's edges to collapse into the centre, shrinking the wound. In order to re-epithelize the wound surface, epithelial cells start to multiply and replace dead cells in the third stage [20, 21].
1.4.4 Maturation Phase/ Remodeling phase
At this point, the freshly created tissue starts to get stronger and more flexible, eventually becoming the first healthy tissue. Tensile strength will increases (albeit the maximal strength is only 80% of the pre-injured strength), collagen fibers are reorganized, and the tissue remodels and develops. Each wound grows in a completely different way [20, 21]. In order to achieve the best possible healing and closure quality, wound care should be taken that is wound free of germs to avoid infection [22], reduce discomfort, and encourage quick healing [23]. Acute wounds that heal in 7-10days become chronic wounds that need prolonged hospital stays and treatment because of the sluggish healing process [24].
Gels, lotions, ointments, dressings, and solutions are examples of commercial products. These therapies, which are primarily based on the concept of moisture intake and are intended to encourage tissue regeneration, are not anti-infective and cannot be utilized in the presence of a potential infection [25]. Additionally, coverings usually cause damage when removed, and traditional therapies can take longer to heal wounds, which means they do not give the optimal conditions for wound recovery. In order to maintain wound sterility, the therapeutic effect of medications, and prevent wound drying, they must also be applied and coated often [26]. Consequently, they reduce patient acceptance and compliance [27]. Because they function as distinct entities that differ from free medications [29], nanocarriers have been shown to enhance therapeutic impact more than drugs themselves [28, 26]. They improve drug transport into the skin by improving pharmacokinetics and biodistribution, which raises the bioavailability of pharmaceuticals [27]. Additionally, they regulate wound infection and inflammation, improve tissue regeneration, lessen wound pain, and encourage wound closure. Since vesicular nanocarriers are the most often described systems for wound healing.
1.5 Factors affecting and Causes of wound healing
Growth factors, cytokines, extracellular matrix, and blood cells collectively contribute to the wound healing process. Cytokines support healing by stimulating inflammation, promoting granulation tissue formation, and enhancing basement membrane synthesis. These pathways are influenced by a variety of local and systemic factors[30]. Local factors such as cold, pain, infection, radiation and tissue oxygen tension, directly affect the features of the wound, whereas systemic factors include an individual's general health or sickness status that affects their ability to heal [31]. Aging, poor diet, and deficits in protein, vitamins, and minerals can all lengthen the healing process.
Causes of delayed wound healing: An acute wound typically takes five days to two weeks to heal during the proliferative phase of the wound-healing cycle, which is followed by a remodeling phase that may extend for two years. However, if there is a deviation from the normal healing pathway and an anomaly in the physiological healing system, it can cease in one of the phases. Because this kind of illness usually does not go through a systematic procedure for regular wound healing, it is referred to as chronic, nonhealing wounds in the wound-healing category. Persistent bacterial proteins, chronic inflammation, wound infection and insufficient blood supply are the primary causes of such delayed wound healing [32].
2. CHALLENGES IN TOPICAL DRUG DELIVERY
Topical drug delivery is widely preferred because it is simple, non-invasive, and easy to apply. It is particularly useful for treating skin infections and localized conditions. However, the primary limitation is the skin barrier, which restricts the entry of many drugs into deeper layers. As a result, conventional formulations often show poor drug penetration and limited effectiveness. [33-40]
3. VESICULAR DRUG DELIVERY SYSTEMS
Vesicular drug delivery systems are composed of lipid-based carriers that can encapsulate drugs and improve their delivery in to the skin. These systems help protect the drug enhance its stability, and allow controlled release. Some of the examples are liposomes, niosomes, ethosomes and transfersomes.
Compared to conventional formulations, vesicular systems improve drug penetration and reduce side effects. They also help in targeting the drug to specific areas, which enhances therapeutic effectiveness. Due to these advantages, they are widely used in wound healing applications [43,44].
3.1 NEED FOR ADVANCED VESICULAR SYSTEMS
Vesicular drug delivery methods are particularly important for targeted drug delivery because they localize the medication's effect at the site or organ of action and lower its concentration at other sections of the body. On the other hand, conventional topical medication delivery methods have inadequate skin deposition and low percutaneous permeability. Scientists can create new vehicles or investigate novel approaches to find better topical products. nanocarriers to guarantee sufficient medication penetration and more crucially, localization in the skin's deeper layers.[45].
4. INTRODUCTION TO TRANSFERSOMES
The Latin word "transferred" and the Greek word "soma" both suggest a "bearing body" in the name. "Soma" refers to a body, whereas "Transfer" literally means to carry.[46, 47]
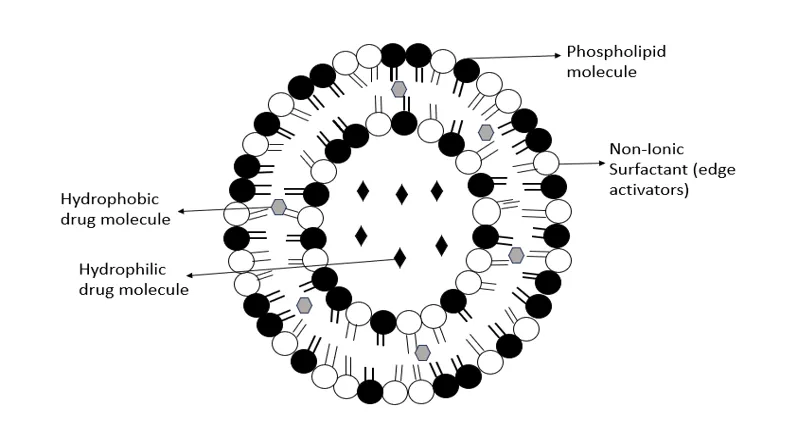
Fig.1 Structure of transfersomes
Early in the 1990s, new lipid vesicles called ultra deformable vesicles (UDV) or deformable or elastic (flexible) liposomes were created. Because UDV are more flexible than traditional liposomes, they have shown a remarkable capacity to penetrate intact skin and transfer the loaded pharmaceuticals into the layers of the dermis and epidermis and even into the systemic circulation. These elastic vesicles were created using phospholipids, ethanol, bile salts, and various surfactants. Two benefits of UDV formulations are nontoxicity and thermodynamic stability. They have been used to transdermally and cutaneously distribute a variety of substances, such as proteins and peptides.[48] Moreover, scaling up their production is simple. Many UDV forms, especially transfersomes, ethosomes, and, more recently, transethosomes, have been effectively created for use in pharmaceuticals and cosmetics.[49]
Transfersomes are flexible vesicular carriers designed to improve transdermal drug delivery. Their structure allows them to change shape and pass through small pores in the skin, enabling deeper penetration. They are mainly composed of phospholipids and surfactants, which provide flexibility and stability. These carriers have been widely studied for delivering various types of drugs, including proteins, peptides and anti-inflammatory agents. Due to their enhanced penetration ability, transfersomes are considered more effective than conventional vesicular systems.[50–55]
4.1 Composition of transferosomes
Transferosomes, a type of vesicular drug delivery mechanism, are composed of a specific ratio of phospholipids, surfactants (edge activators), and water [56]. For example, the phospholipids that make up the bilayer membrane, such phosphatidylcholine, include hydrophilic and lipophilic medications that are buried in the aqueous core and bilayer, respectively. Transferosomes have significant flexibility and elasticity because another component, such as edge activators (such sodium cholate, Tween 80, or Span 80), disrupts and fluidizes the lipid bilayer. Additionally, water promotes medication release after skin contact and helps preserve the structural integrity of the vesicle. These components work together to create ultra-deformable vesicles that can change shape and pass through skin pores that are much smaller than their diameter without rupturing [57].
4.2 Transfersomal delivery of Drugs
Transfersomes shows excellent skin permeability, high drug loading capacity, and regulated release behaviour and making an remarkable promise in enhancing therapeutic efficacy across a wide spectrum of medical conditions. [58, 59]
4.2.1 Delivery of anti?inflammatory and analgesic drugs
Furthermore, transferosomes have shown improved therapeutic efficacy for the transdermal and cutaneous delivery of anti-inflammatory drugs. For example, diclofenac sodium-loaded transferosomes (3%) demonstrated a roughly 2.8-fold improvement in epidermal penetration and a 60% better reduction in paw edema in an animal model when compared to commercially available gels of similar concentrations [60]. The therapeutic efficacy of ibuprofen-loaded transferosomal gels was three and a half times greater than that of traditional topical preparations. The increased effectiveness of medications administered via transferosomes is due to the high deformability of vesicles, which maintain structural integrity and survive in the deeper dermal layers, enabling an extended residence period at the site of action [61].
4.2.2 Potential antifungal and antimicrobial uses
Transferosomal compositions for antifungal topical dispersion have been extensively studied. For example, fluconazole-loaded transferosomes demonstrated 85% mycological cure rates in mice infected with Candida, which is significantly greater than the 55–60% cure rates with traditional creams [62]. Similarly, compared to standard formulations, which took 15–18 days to eradicate the infection, clotrimazole transferosomal gels boosted drug deposition in the skin by 4.5 times and did so in 10 days [63]. These results clearly demonstrate the penetrative and retention properties of transferosome formulations, which are crucial when dealing with diseased skin tissues.
4.2.3 Delivery of vaccines and peptides
Transferosomes are an intriguing novel delivery system for transcutaneous vaccination. A transferosomal formulation of hepatitis B antigen generated 1.8 times greater antibody titers than intramuscular injection [64]. Insulin-loaded transferosomes and a transferosomal oxytocin system, which sustained therapeutic drug concentrations in plasma for prolonged periods of time to lower dosage and improve patient compliance, also enabled effective transdermal drug administration [65]. Collectively, these studies show that transferosomes can assist in the transdermal transport of large and small biomolecules across the epidermal barrier.
4.2.4 Delivery of Antioxidants
Transfersomes also been explored for the delivery of antioxidant molecules used in skin protection and wound healing. Antioxidants such as resveratrol, epigallocatechin gallate and curcumin have demonstrated improved skin permeation and enhanced therapeutic activity when incorporated into transfersomal systems. These formulations help to reduce oxidative stress, accelerate tissue regeneration and promote collagen synthesis during the wound healing process [64, 65, 66, 67].
4.2.5 Delivery of herbal drugs
In herbal formulation included a surface-active ingredient that improve drug penetration through the stratum corneum. For example, transfersomes of capsaicin that showed superior topical absorption over pure capsaicin. Because of their anti-inflammatory qualities, which also ensure better drug absorption, curcumin transfersomes are used [68].
5. MECHANISM OF PENETRATION OF TRANSFERSOMES
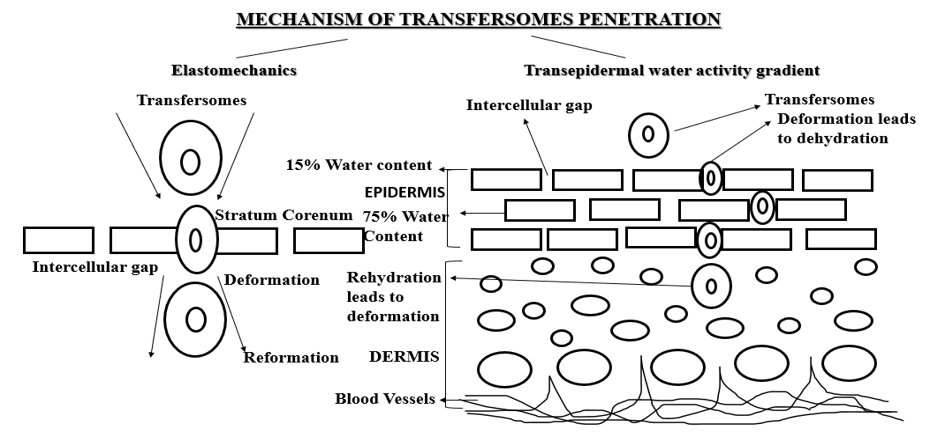
Fig.2 Mechanism of Transfersomes Penetration
Transfersomes penetrate through the skin by adapting their shape and moving through the spaces between skin cells. Their flexible structure allows them to pass through narrow pathways and finally reach deeper skin layers. This helps in delivering the drug effectively at the target site and improves its therapeutic action [69-72]
6. METHODS OF PREPARATION OF TRANSFERSOMES
In this technique, the vesicle preparation procedure consists of three steps. Phospholipids and surfactants are added to a round-bottom flask, then it is immersed in a solution of methanol and chloroform to evaporate the solvent and create thin film vesicles. It is necessary to heat the created thin film above the transition temperature of the lipids. To remove any leftover detergent, place the generated film under vacuum for the whole night after the solvent has been evaporated using a rotary evaporator. Secondly, use a buffer which is used to hydrate the film by spinning it at 60 rpm for an hour and then allowing it to swell for two hours at room temperature. Finally, sonicate the vesicles (2.0 mL of 30% aqueous foam) by using a probe sonicator. Extrude the sonicated vesicles ten times through 200 nm and then 100 nm polycarbonate membranes to obtain the desired vesicle size [73,74].
In this technique, phospholipids and edge activators are dissolved in ethanol and slowly injected into an aqueous phase containing the drug under continuous stirring. As ethanol diffuses into the aqueous medium, vesicles are spontaneously formed. This method is simple, rapid, and suitable for preparing small-sized transfersomes with good uniformity [75,76].
Lipid samples are combined with edge activators in the aqueous phase, and then nitrogen is purged in the round-bottom flask. Depending on the solubility characteristics, the medication is added to either the aqueous phase or the lipid phase. Then two combined phases are sonicated for at least half an hour to create a homogenous, stable dispersion. The organic component is then removed at a reduced pressure, leaving the original combination with a thick gel-like substance that will eventually form the vesicles needed to ensure drug delivery. The pharmaceutically ready product can next be separated using dialysis or centrifugation, removing any remaining solvent and non-encapsulated material [77, 78].
In this process, the drug will be combined with phosphatidylcholine and edge activators to make a homogeneous solution, then it will be dissolved in a 1:1 ethanol:chloroform solvent mixture. The organic solvents will be removed by whirling at a temperature higher than the lipid transition temperature (about 43 °C) until a thin uniform layer is clearly visible on the inside walls of the flask. Finally, the transferosome film will be allowed to equilibrate for an entire night to stabilize the vesicular formulation and enable complete solvent evaporation [79]. A phosphate buffer (pH 6.4) will be used to rehydrate the dried films following an overnight incubation period. In order to give the dry films enough time for intermolecular contacts and the formation of a stable sus pension, the phosphate buffer will be applied gradually while gentle agitation is maintained for 15 minutes at the predefined temperature. A second rehydration step will be carried out, during which the transferosome suspension will be hypothermally incubated for one hour. This will primarily maintain the temperature between 2 and 8 °C, giving the transferosomes the time they need to self-assemble and stabilize the colloidal system [80].
Table.2 Principles, advantages, disadvantages and Entrapment efficiency of Methods
|
Method |
Principle/process |
Advantages |
Disadvantages |
Entrapment Efficiency |
|
Thin film hydration technique |
Lipids and surfactants dissolve in an organic solvent under well watched circumstances, evaporate to form a thin lipid film, and then be hydrated with an aqueous drug solution. |
High drug loading for both lipophilic and hydrophilic drugs is made possible by its popularity, ease of usage, and repeatability. |
Solvent removal is necessary because heat-sensitive components could oxidize or break down. |
Good vesicle homogeneity and a high yield (80–90%)
|
|
Ethanol injection technique |
Vesicles naturally occur when ethanol diffuses after an ethanol lipid solution is introduced into an aqueous medication solution while being agitated. |
Easy, quick, low heat; generates little vesicles
|
Remaining ethanol may have an effect on limited scalability and stability. |
Moderate yield (70–80%) with vesicles smaller than 200 nm
|
|
Reverse phase evaporation method |
A water-in-oil emulsion is made using lipid in the organic phase and an aqueous drug solution; solvent evaporation leads to vesicle formation. |
Huge unilamellar vesicles that effectively encapsulate hydrophilic macromolecules
|
necessitates the use of organic solvents; possible toxicity or instability issues
|
High yield (> 90%), 200–500 nm unilamellar vesicles
|
|
Modified hand-shaking method |
Similar to thin film hydration, however instead of using rotary evaporation for small-scale formulation preparation, manual shaking or vortexing is employed. |
Easy, reasonably priced, and suitable for preliminary screening
|
Poor batch reproducibility and a broader range of vesicle sizes
|
Greater vesicle diameters (> 300 nm), moderate yield (60–75%)
|
7. CHARACTERIZATION PARAMETERS
The vesicle size distribution, and zeta potential in respect to the dispersion are measured using the DLS system of our Malvern Zeta sizer. By monitoring the light scattering from particles suspended in solution caused by laser technology, the DLS system as certain the size and other characteristics of the vesicles. For each of these parameters, accurate values were discovered. Based on the testing, it could evaluate and understand their stoichiometry and stability under different situations [81].
Vesicle morphology is commonly evaluated using transmission electron microscopy (TEM) or scanning electron microscopy (SEM). These techniques provide detailed information regarding the shape, surface characteristics, and structural integrity of transfersomes. Most transfersomal vesicles appear spherical with smooth surfaces and uniform distribution [82].
The amount of drug trapped in the formulation is indicated by the entrapment efficiency (%EE). To determine the EE, the unentrapped drug is recovered from the vesicles using a number of techniques. Both direct and indirect methods can be used to determine %EE in this process. The direct procedure would entail emptying the supernatant after ultracentrifugation and then using an appropriate solvent that can be analyse the sediment to rupture the sedimented vesicles. The resulting solution can then be diluted and filtered through a syringe filter (0.22–0.45 µm) to remove the impurities. The drug content is determined by using analytical methods such as spectrophotometry or modified high-performance liquid chromatography (HPLC) depending on the active pharmaceutical ingredient (API) [83,84,85]. The entrapment efficiency, or percentage of drug entrapment, is expressed as:
%Entrapment efficiency = Amount of the drug entrapped/ Total amount of the drug added ×100
The indirect approach for calculating the %EE involves diluting the supernatant with a suitable solvent and filtering it to remove the impurities. The amount of the drug in the supernatant is determined as the free drug using an appropriate analytical method. Therefore, the expression for the percentage of drug entrapment is as follows:
%Entrapment efficiency = Total amount of the drug added − Amount of free drug / Total amount of the drug added ×100
Permeability is an important characterization parameter and a unique measurement for transfersome study in the future. The Permeability of transfersomes was tested using pure water as a control. The formulation was passed through a series of microporous filters with pore sizes varying from 50 to 400 nm, depending on the original transfersome solution. Particle size and size distributions were examined using DLS measurements following each filtration pass.
Formula can be used to determine the degree of deformability is:
D = J × rv/rp
In this formula, rv is the vesicle size, rp is the barrier's pore size, and J is the volume of suspension extruded in five minutes [86,87,88].
This value is important since it affects the penetration of the transfersomal formulation. In this study, pure water serves as the standard. The preparation is filtered through a variety of microporous filters with known pore sizes ranging from 50 to 400 nm. Particle size and size distribution are recorded using DLS measurements after each pass [89,90,91].
Turbidity measurement is used to evaluate the clarity and homogeneity of transfersomal dispersions. It indirectly indicates vesicle size distribution and aggregation behavior. Increased turbidity may suggest particle instability within the formulation [89,90,91].
Fluorescence microscopy allows for the evaluation of transfersomes ability to cross cellular membranes. This biological testing will define the range of movement that transfersomes, as a therapeutic delivery method, can have across biological barriers to deliver the therapeutic material. [93]
A modified high-performance liquid chromatography (HPLC) can be used to assess the drug content precisely. An UV detector is used to quantify the amount of light absorbed, giving the researcher a precise assessment of the active medicinal ingredient under investigation. Using an autosampler in this HPLC method lowers human error because the autosampler automatically injects the samples and the column oven regulates the temperature. Following the pump's passage of the sample and mobile phase through the column, the computer program measures the data. This strategy is effective and essential for the efficacy and safety of the pharmaceutical products being developed [94–96].
In vitro drug release studies of drug penetration through skin-like barriers often employ Franz diffusion cells. The donor compartment, which contains the drug formulation, is taped to the receptor chamber, and the fluids in the receptor chamber are continuously stirred by a magnetic stir bar to aid in fluid mixing [97]. The average skin temperature in vivo is 32 ± 1 °C, which is also the temperature of the receptor fluid. The membranes are made of mixed cellulose esters and have an average pore size of 0.45 μm. The membranes were initially wetted with phosphate buffer and kept at room temperature for the whole night in order to allow the membrane pores to enlarge and so improve permeability [98]. Using specific time points (0, 0.5, 1, 2, 3, 4, 5, and 6 h), a volume of 1 mL was removed from the receptor medium and replaced with 1 mL of phosphate buffered saline (PBS) in order to maintain sink conditions. The aliquots of receptor media were concentrated, and the drug concentration was determined using a UV spectrophotometer with a defined absorbance in order to produce an elution profile release and skin penetration properties of the experimental drug formulation [99].
Permeation experiments are conducted to prevent transdermal medication distribution using an in vitro Franz diffusion cell model. In accordance with the protocol, proprietary membranes will be fitted with the stratum corneum to the donor compartments, and PBS, a biocompatible medium, will be utilized to replicate continuous circumstances. Each donor compartment will store a predetermined volume of the test formulation, which will promote diffusion under non-occluded conditions, like in practice. At predefined intervals, the volume of the receptor medium will be removed and replaced with fresh PBS to account for sink conditions and reduce data loss from evaporation. A validated UV spectrophotometer will be used to assess the drug's absorption in the receptor media in order to determine the transdermal permeation profile of the test formulation [100–102].
Transfersomes are evaluated for stability using transmission electron microscopy (TEM) at 4 and 37 °C as particular drug delivery vehicles. Additionally, dynamic light scattering (DLS) measurements will be performed 30, 45, and 60 days following preparation to assess size changes that may indicate instability. The initial drug entrapment value will be set at 100% and the percentage of drug loss will be computed in order to evaluate the formulations' overall viability. The best transdermal preparations should be stored in amber vials with tight-fitting covers to protect them from light [103,104]. Important characterization criteria for evaluating transferosomal formulations are included in Table 2 together with sample data ranges for topical treatments.
CONCLUSION:
In conclusion, transfersomes offer a modern and effective approach for improving wound healing. Unlike traditional topical formulations, they can penetrate deeper into the skin due to their flexible structure, allowing better delivery of drugs at the required site. This leads to improved therapeutic outcomes, faster healing and reduced side effects.
Their ability to carry different types of drugs and herbal products including synthetic compounds, makes them highly useful in wound care treatment. Transfersomes also help in enhancing drug absorption, maintaining drug concentration at the target site, and supporting tissue repair processes.
Although there are some limitations such as stability and production challenges, ongoing research is continuously improving their performance. Overall, transfersomes have strong potential to become an important part of advanced wound healing therapies in the future.
REFERENCES

Velpuri Nikitha Lakshmi, Vothani Sarath Babu, Chinnaguravagari Saranya, Transfersomal Nanocarriers for Enhanced Wound Healing and Transdermal Drug Delivery: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 4048-4065. https://doi.org/10.5281/zenodo.20727577
 10.5281/zenodo.20727577
10.5281/zenodo.20727577