
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Karnataka College of Pharmacy Bengaluru-560064.
Rheumatoid Arthritis (RA) is an autoimmune, chronic systemic disease that involves synovial inflammation, progressive joint damage and related extra-articular manifestations. Although pharmacological therapy has improved, traditional therapies have limitations, such as systemic side effects, inefficacy and expense. The evolution of new drug delivery systems, especially niosomal gels, has proven to be a highly effective way to increase the localized and sustained cure of RA. Niosomes are surfactant-based non-ionic vesicles which enhance drug bioavailability, stability and targeted delivery. When formulated with a transdermal gel, niosomes offer controlled release of drugs, enhance drug permeation across the skin and reduce systemic side effects. The present review exhaustively presents the pathogenesis of RA, existing treatment strategies and the potential of niosomal gel-based drug delivery in RA therapy. It also discusses recent developments, formulation approaches, critical evaluation parameters and issues related to niosomal technology. Future research directions include the optimization of formulation stability, investigating combination therapy and developing applications for other inflammatory conditions. Niosomal gels show great promise as an alternative to traditional therapy, promising better patient compliance and efficacy in the management of RA.
Rheumatoid Arthritis (RA) is a chronic systemic autoimmune inflammatory disorder that is marked by inflammation of the synovial membrane, resulting in progressive cartilage destruction of articular cartilage, bone erosion and associated deformities and extra-articular manifestation of disease [1]. The prevalence of RA worldwide has been estimated to be around 1%, and the incidence of RA in females is two to three times higher than in men [2]. Though RA can influence individuals of every age, middle-aged individuals aged 30-50 years have a higher rate of RA[3]. Each year for every 1,00,000 individuals, 41people are diagnosed with RA [4]. Though lots of progress in the management of RA has taken place, therapy today still is limited by certain drawbacks such as systemic side effects, suboptimal efficacy, and excessive expenses. In recent years, there has been an increasing interest in the creation of new drug delivery systems that can deliver targeted, sustained, and safe RA treatment. [5] Liposomes were initial vesicular drug delivery systems but they possess numerous drawbacks like toxicity, and pH dependent stability, therefore due to this reason the interest in research moved towards Niosomes. [6] Niosomes are ionic surfactant vesicles created by the self-assembly of non-ionic amphiphiles in aqueous systems leading to closed bilayered structures. Niosomal gel, a topical drug delivery system, has shown great promise in the treatment of RA. Niosomal gels are able to withstand the physiological stress developed due to skin flexion and thus extend controlled release of the drug to the site of action. [7] The gel drug delivery system offers an easy and patient-friendly delivery platform for transdermal administration, enabling localized therapy of involved joints.
The precise mechanism of RA is not known, studies have however outlined some major factors responsible for the etiology of the disease. These factors broadly fall under two broad categories: genetic factors and environmental factors. [8]
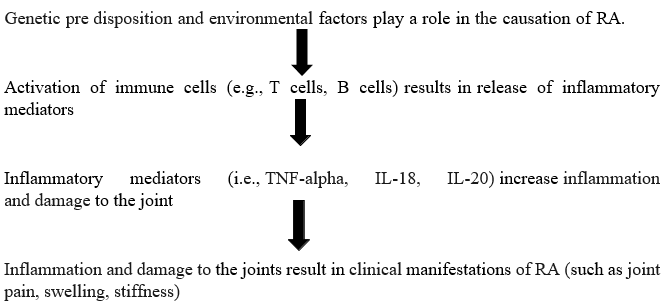
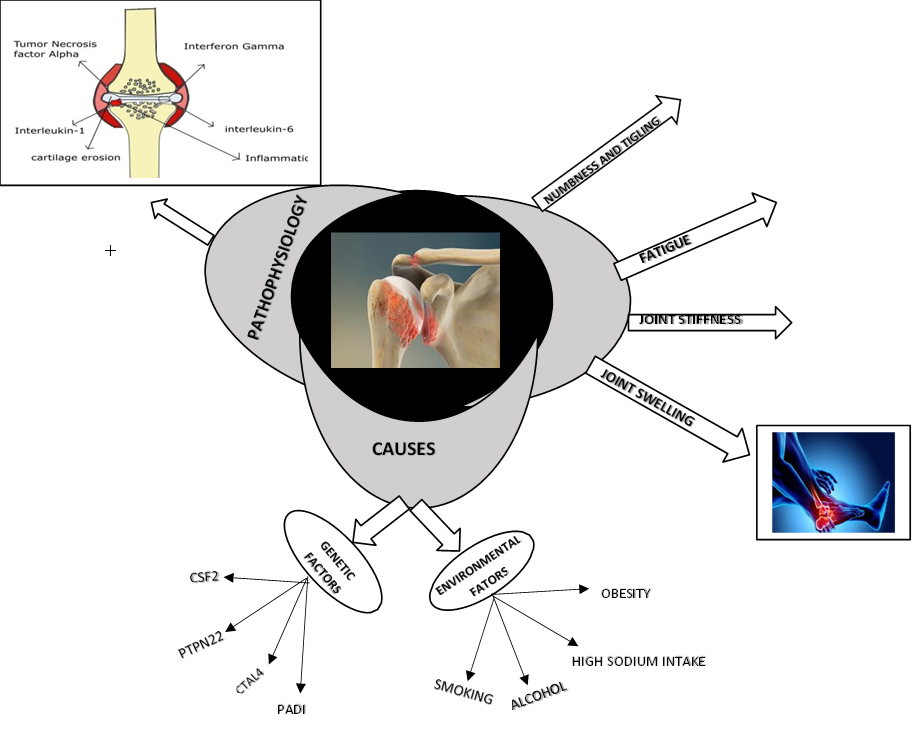
Fig No 1: Factors influencing pathogenesis of rheumatoid arthritis
Treatment Approaches for Rheumatoid Arthritis
Table No.1: Treatment approaches for Rheumatoid Arthritis
|
Sr. No |
Dosage form |
Class of Drug |
Drug |
Mechanism of Action |
Ref |
|
|
1. |
Tablets |
NSAIDs |
Celecoxib |
Selective inhibition of COX-2 |
[9] |
|
|
2. |
Capsules |
DMARDs |
Sulfasalazine |
Inhibits dihydrofolate reductase |
|
[10] |
|
|
|
NSAIDs |
Indomethacin |
Inhibition of prostaglandins, inflammatory and anti-pyretic |
anti- |
[11] |
|
3. |
Liquid Orals |
DMARDs |
Azathioprine |
Immunosuppressant, inhibits de novo pathway of purine synthesis and thus prevents the DNA replication Process |
[12] |
|
|
4. |
Topicals |
DMARDs |
Methotrexate |
Inhibits aminoimidazole carboxamide ribonucleotide (AICAR) transformylase and thymidylate Synthetase |
[13] |
|
|
5. |
Transdermal Patches |
NSAIDs |
Diclofenac sodium |
Inhibits prostaglandins and synthesis |
COX |
[14] |
Novel Nanocarriers for management of Rheumatoid Arthritis.
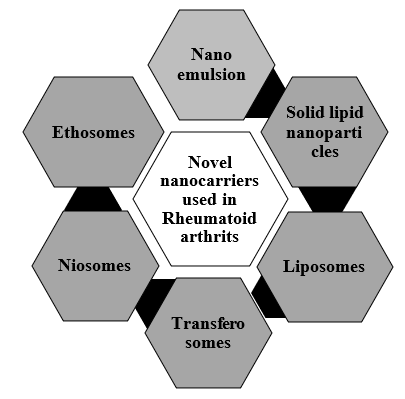
Fig No.2: Novel Nanocarriers for management of Rheumatoid Arthritis.
Characteristic features of nanocarriers
Table No.2: Characteristic features of nanocarriers
|
Carrier |
Characteristic features |
Advantage |
Disadvantage |
Ref. |
|
Nano emulsions |
|
|
|
[15,16 ,17,18] |
|
Solid lipid nanoparticles (SLNs) |
.
|
|
transition upon sto rage |
[19,20 ,21] |
|
|
|
|
Recent Patents on Nanocarrier for Rheumatoid Arthritis
Table No.3: Recent Patents on Nanocarrier for Rheumatoid Arthritis
|
Application Number |
Tittle of Inventions |
Summary of the Invention |
Ref |
|
AU 2014234992 B2 |
Methods for treating inflammation, autoimmune disorders and pain |
This invention describes methods for the prevention of oral mucositis, inflammatory bowel diseases. The above kits are developed along with respective guidelines for administering a therapeutically effective dose of cationic steroid antimicrobial. |
[33] |
|
US 2015/0174069A1 |
Methods of Treating Arthritis |
The Invention Pertains to the treatments for arthritis, which inclu de administering a sustained release composition that contains liposomes consisting of one or more phospholipids, cholesterol, and an active drug. |
[34] |
|
US 20170260276 |
Treatment for Rheumatoid arthritis |
This revelation is in reference to the treatment of rheumatoid arthritis through inhibiting biological activity of granulocyte/macrophage colony stimulator factor receptor alpha subunit (GM-CSFRα), through the administration of an inhibitor like the therapeutic antibody mavrilimumab. |
[35] |
|
US20220349885 |
Biomarker for diagnosing rheumatoid arthritis and uses thereof |
The invention involves marker composition for diagnosing rheumatoid arthritis through angiotensinogen (ACT). It consists of a method to detect rheumatoid arthritis, a composition for measuring the markers expression, and a detection kit. The method allows one to make a precise diagnosis sin joint disease such as rheumatoid arthritis. |
[36] |
|
US 20210341491A1 |
Rheumatoid arthritis auto- antibody-bound peptide and application thereof |
This invention involves peptide that binds to rheumatoid arthritis autoantibodies and also provides a testing method and reagent kit to determine whether a subject is affected by rheumatoid arthritis. |
[37] |
|
WO2019009231 A1 |
Diagnostic of rheumatoid arthritis |
The invention provides a method for diagnosing rheumatoid arthritis, an auxiliary diagnosis, and monitoring disease activity and therapeutic effects of a drug. |
[38] |
Niosomes:
Structure of Niosomes:
Fig No.3: Structure of Niosomes
Niosomes are the bi-layered nature of non-ionic surface- active agents. These thermodynamically stable bi- layered entities are developed only when surfactants and cholesterol are blended in a proper ratio, and the temperature is greater than the temperature of gel liquid transition [39]. There remains an empty space in the middle of this two-layered nature. The distinctive shape of Niosomes allows them to enclose hydrophilic and hydrophobic drugs inside their structure. Hydrophilic drugs may be adsorbed on the bilayer surface or entrapped in the central watery core of niosomes, while hydrophobic drugs partition in the bilayer matrix to enter it [40]. The bilayer matrix of the niosome is described with the aid of Figure, where it is easy to identify the two distinct regions for drug entrapment.
Formulation components of Niosomes
Niosomes are composed of several key components that contribute to their structure and functionality as drug delivery systems. The main components include:
Non-ionic Surfactants
Non-ionic surfactants are uncharged amphiphilic molecules. They are the most significant components of niosomes, which self-assemble into bilayer formations in an aqueous system. Span (sorbitan esters) and Tween (polysorbates) are some of the typical non-ionic surfactants that find application in niosome formulation. The surfactants stabilize the vesicles and can entrap both lipophilic and hydrophilic drugs. They allow the formation of vesicles by lowering the surface tension between the lipid phase and aqueous phase, hence allowing the niosomal structure to form stable structures [41,42,43].
Cholesterol:
Cholesterol is commonly incorporated in the niosomal bilayer to enhance the stability of the membrane. It is considered a "mortar" that closes spaces between surfactant molecules, thereby strengthening the bilayer. Cholesterol addition can decrease membrane fluidity, enhance stability, and alter membrane permeability, which can increase the entrapment efficiency of drugs in niosomes. Cholesterol is required for the structural stability of niosomes, particularly under fluctuating environmental conditions [44, 45, 46].
Charged molecule:
Charged Molecule are those additives that introduce a positive or negative charge to the niosomal surface. This can help in stabilizing the vesicles and also affects their interaction with biological membranes. The most commonly used charge inducers are stearyl amine, which introduces a positive charge, and dicetyl phosphate, which introduces a negative charge. These charge inducers can prevent the aggregation of niosomes, prolong their circulation time in the bloodstream, and enhance the delivery of negatively charged drugs, such as polynucleotides, into cells [47,48,49].
Types of Niosomes
Niosomes can be classified based on their size into three main categories:
1. Small Uni-lamellar Vesicles (SUVs): These have a size range of 10–100 nm.
2. Large Uni-lamellar Vesicles (LUVs): These range from 100–3000 nm in size.
3. Multilamellar Vesicles (MLVs): These contain more than one bilayer[50,51,52]
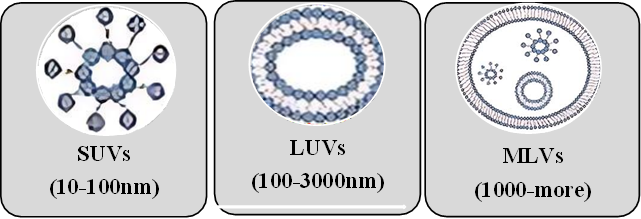
Fig No.4: Types of Niosomes
Other Special Niosomes:
Niosomal Gel as a Drug Delivery System
Niosomes in drug delivery
Niosomal gels are a potent drug delivery system owing to their capacity for encapsulating a broad spectrum of therapeutic drugs, ranging from hydrophilic to hydrophobic and amphiphilic agents. This is because of the structural nature of Niosomes, which are bilayer vesicles derived from non-ionic surfactants [65]. The vesicles are capable of trapping hydrophilic (water-soluble) as well as hydrophobic (fat-soluble) drugs, thus enhancing the bioavailability and therapeutic activity of the entrapped agents.
Encapsulation of Hydrophilic Compounds: Niosomes are able to encapsulate water-soluble drugs within their aqueous core and are thus suitable for targeted delivery and prolonged release. This is especially useful for drugs that need extended action on the site of administration [66].
Encapsulation of Hydrophobic Compounds: The lipid bilayer of Niosomes provides a suitable environment for hydrophobic drugs, which can be incorporated into the membrane. This capability allows for the delivery of a broader range of therapeutic agents, including those that are poorly soluble in water [67].
Amphiphilic Compounds: Niosomes can also encapsulate amphiphilic compounds that have both hydrophilic and hydrophobic properties. This flexibility in encapsulation enhances the stability and efficacy of the formulation [68].
Mechanism of Niosomal gel action:
The mechanism of niosomal gel action involves several interconnected processes that enhance drug delivery through the skin. Initially, niosomes are formed from surfactants such as AOT (anionic) and Pluronic L64 (non-ionic), which create lamellar liquid crystalline (LLC) phases that encapsulate drugs, allowing for controlled release and improved stability [69]. When applied to the skin, these niosomal gel systems facilitate the permeation of drugs through the stratum corneum, the outermost layer of the skin. The niosomes enhance skin hydration and lipid fluidization, which are critical for improving drug absorption [70]. Additionally, the positive charge of certain drugs, like propranolol, interacts favourably with the negatively charged skin membrane, further enhancing permeation. The formulations are designed for sustained drug release, as the drug must diffuse through the gel matrix to reach the skin, providing a controlled delivery mechanism [71]. Importantly, these gel-niosomes systems have shown to be stable over time, with no sedimentation or flocculation, ensuring their effectiveness [72]. Overall, they act as effective permeation enhancers compared to free drug solutions, making them promising candidates for transdermal drug delivery applications.
Advantages of Niosomal gel over other formulation
Niosomal gel combines the benefits of niosomes with the ease of gel formulations, offering advantages over oral, topical, and other vesicular systems such as liposomes and ethosomes.
1. Improved Drug Stability: Niosomes consist of a mixture of non-ionic surfactants that are more stable than liposomes, which are prone to oxidative degradation. Incorporation of niosomes into a gel matrix stabilizes the vesicles to the full extent by preventing aggregation and leakage and hence maintaining integrity along with efficacy of the drug being encapsulated [73].
2. Improved Skin Penetration: Niosomal gels have been demonstrated to increase drug permeation across the skin barrier. For instance, a study on azithromycin-loaded niosomal gel indicated increased skin penetration and retention when compared with the standard formulation. This indicates that niosomal gels may be applied to enhancing topical drug delivery [74].
3. Avoidance of Systemic Side Effects: Topical use of niosomal gels ensures localized drug delivery, thus minimizing systemic absorption and side effects that might be seen with oral routes. Topical use gives increased drug concentration at the site of action with decreased systemic exposure [75].
4. Controlled and Prolonged Release: Niosomal gels facilitate controlled and prolonged release of the drug entrapped within. Development of a niosomal gel for lopinavir transdermal delivery exhibited a slow release profile of the drug, which is desirable as it achieves therapeutic levels of the drug for a longer duration relative to conventional immediate-release oral products [76].
5. Cost-Effectiveness: The preparation of niosomes requires non-ionic surfactants which are less costly compared to the phospholipids required for liposome formulation. The chemical stability is also higher in niosomes, which reduces the processes that are associated with expensive stabilization methods[77].
6. Enhanced Patient Compliance: The gel form of niosomal formulations is consumer- friendly, not greasy and easy to apply. The treatment compliance is better as the product reduces the need for frequent applications due to the sustained release characteristic [78].
7. Minimized Irritation: Niosomal gels contain biocompatible and non-immunogenic surfactants, which minimize the risk of skin irritation and allergic reaction. This is a significant advantage over other vesicular systems that might contain irritant components [79].
Comparison Table: Niosomal Gel vs. Oral, Topical and Vesicular Systems
Table No.4: Comparison Table: Niosomal Gel vs. Oral, Topical and Vesicular Systems
|
Feature |
Niosomal Gel |
Oral Formulations |
Topical (Non- vesicular) |
(Liposomes, Ethosomes) |
|
Stability |
High |
High |
Moderate |
Low to Moderate |
|
Skin penetration |
High |
None |
Limited to Superficial layers |
Moderate (Liposomes) High (Ethosomes) |
|
Avoids First-Pass |
Yes |
No |
Yes |
Yes |
|
Controlled Release |
Yes |
No |
No |
Yes (Limited by stability) |
|
Cost |
Moderate |
Low |
Low |
High |
|
Patient Compliance |
High |
Moderate |
High |
Moderate |
|
Irritation Potential |
Low |
Moderate (Systemic side effects) |
Low to Moderate |
Moderate to High (Ethosomes) |
Role of Niosomal gel in managing Rheumatoid Arthritis
Role of Transdermal formulation in Managing Rheumatoid Arthritis
Transdermal formulations play a very significant role in the management of RA, as they allow for local drug delivery, thus decreasing systemic side effects and improving the therapeutic outcome of treatment. Drugs delivered through the skin avoid the first-pass effect upon the liver, increase bioavailability, and permit sustained levels of therapeutic drugs at the site. Targeting the inflamed joints through a transdermal system decreases systemic exposure and usually reduces gastrointestinal, renal, and cardiovascular side effects characteristically attributed to oral therapies [80]. Additionally, transdermal systems provide sustained and controlled drug release, maintaining effective drug concentrations over extended periods and reducing the need for frequent dosing. Transdermal delivery significantly improves patient compliance, as it is non-invasive, easy to apply and eliminates the need for daily oral administration. Advanced transdermal technologies, such as niosomal gels and patches, also enhance drug penetration and accumulation in affected tissues, further optimizing RA management [81].
Anti-inflammatory and Analgesic Agents
I. Corticosteroids:
Corticosteroids are widely used for their anti-inflammatory properties in rheumatoid arthritis. They have distinct pharmacokinetic and pharmacodynamic characteristics. Pharmacokinetically, they can be administered through various routes, such as oral or intravenous administration, with good absorption and wide distribution throughout the body due to their lipophilicity. They are primarily metabolized by the liver and excreted by the kidneys, with a variable half-life depending on the specific corticosteroid. Pharmacodynamically, corticosteroids work by binding to glucocorticoid receptors, thus suppressing pro-inflammatory mediators such as TNF- α and IL-6, preventing leukocyte infiltration, and decreasing the production of immunoglobulins[82,83,84].
II. Disease-modifying antirheumatic drugs: Disease-modifying anti-rheumatic Drugs (DMARDs) are also used in the treatment of rheumatoid arthritis. Their pharmacokinetics are different, and some are given orally, while others are injected or infused, which alters their absorption rate. Tissue distribution of DMARDs is generally uniform, although some concentrate in specific organs, like methotrexate in the liver. They are all metabolized by the liver, and renal excretion is common. Pharmacodynamically, DMARDs act through the immune response by inhibiting the proliferation of activated lymphocytes and the production of inflammatory cytokines, thus preventing damage to the joint and maintaining function over time[85].
III. Biological agents: Biological agents, a more targeted approach in RA treatment, also have particular pharmacokinetic properties. These agents are typically administered subcutaneously or intravenously, varying their bioavailability by method. Due to their larger molecular size, they have a limited distribution volume compared to traditional small-molecule drugs. They are metabolized through proteolytic degradation and are excreted mainly via the reticuloendothelial system and kidneys. On the pharmacodynamic front, biological agents specifically target molecular mediators of inflammation, such as inhibiting TNF-α, which leads to a marked decrease in inflammatory signals and the overall immunological response, reducing the activity of B and T cells involved in the disease process. This integrated understanding of their pharmacokinetic and pharmacodynamic properties helps inform their clinical application in the treatment of rheumatoid arthritis[86,87,88].
Niosomal gel formulation
Preparation methods
1) Ether Injection Method
2) Hand Shaking Method (Thin Film Hydration Technique)
3) Sonication Method
4) Formation of Niosomes from Proniosomes
5) Micro Fluidization
6) Multiple Membrane Extrusion Method
7) Reverse Phase Evaporation Technique (REV)
8) Freeze-Thawing Method
9) Bubble Method
Ether Injection method:
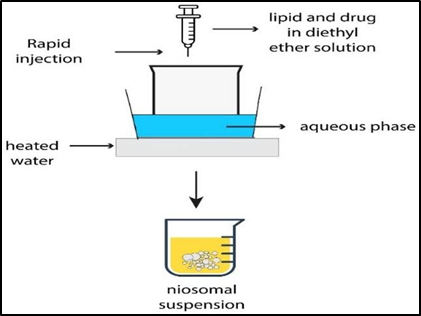
Fig No.5: Ether Injection method
The fd Ether Injection The steps in preparation of niosomes by ether injection are as follows. Initially, surfactant solution is prepared by dissolving desired non-ionic surfactant in diethyl ether. Second, warm water is maintained around 60°C in a proper container. Finally, surfactant solution is injected slowly into the warm water through a 14-gauge needle. When the ether is added to the aqueous phase, owing to the high temperature, it evaporates at once and promotes the self-assembly of surfactant molecules into vesicular structures, resulting in single-layered niosomes, diameters between 50 and 1000 nanometres depending on certain conditions like temperature and concentration of surfactant [89].
Hand Shaking Method (Thin Film Hydration Technique):
Fig No.6: Thin film hydration technique
Preparation of niosomes by Thin Film Hydration Method is a systematic process initiated by dissolving an intimate mixture of cholesterol and non-ionic surfactant in a volatile organic solvent, i.e., chloroform or diethyl ether, in a round-bottom flask. Organic solvent is subsequently removed by the process of rotary evaporation at room temperature to produce a thin film of lipid coated on the wall of the flask. After the evaporation of the solvent, the dried surfactant film is rehydrated with an aqueous phase at temperatures between 0°C and 60°C, gently agitating to allow rehydration. This rehydration results in multilamellar Niosomes [90].
Sonication Method:
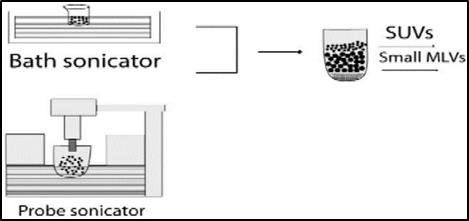
Fig No.7: Sonication Method
sonication procedure for niosome preparation is easy and effective. To start with, a solution of mixture of cholesterol and non-ionic surfactant is made. The solution can also have the drug to be encapsulated in it. Then the solution of surfactant and drug is put into a glass vial, and an adequate buffer is added to achieve the concentration level. The vial is subsequently sonicated in a sonicator with a titanium probe, typically at a controlled temperature of around 60°C. Under sonication, high-frequency sound waves generate shear forces that favour the disruption of surfactant aggregates and hence the formation of niosomal vesicles[91].
Formation of Niosomes from Proniosomes:
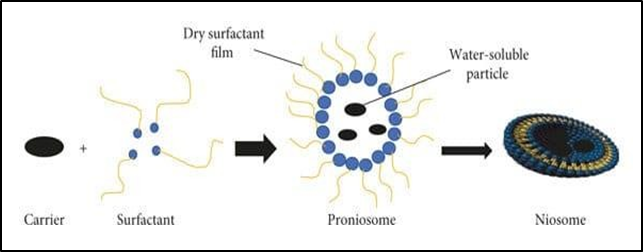
Fig No.8: Formation of Niosomes from Proniosomes
Preparation of niosomes from proniosomes involves a straightforward process of hydration. Proniosomes are powdered free-flowing systems which are a blend of surfactants, cholesterol, and a drug, often coated on a carrier, for example, maltodextrin or other hydrophilic substances. A suitable aqueous phase, typically phosphate buffer or distilled water, must be mixed with the proniosomes along with mild agitation or heat treatment for proniosome-to-niosome conversion. This process also hydrates the surfactant layer, resulting in the self-assembly of niosomes, which are vesicular structures that encapsulate the drug [92].
Micro Fluidization:
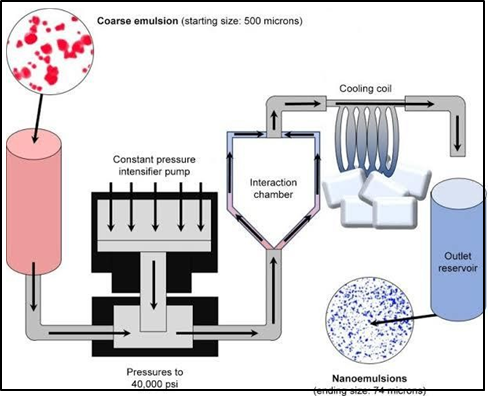
Fig No.9: Micro Fluidization
The preparation of niosomes via the micro fluidization method involves using a high- pressure homogenization technique to yield uniform and reproducible vesicles. In this process, surfactants, cholesterol and the drug are dissolved in suitable organic solvents to form a lipid phase while an aqueous phase (buffer solution) is prepared separately. These two phases are further processed through a microfluidizer in which they are forced to mix under high shear conditions in a microchannel. This interaction gives niosomes a narrow size distribution and high encapsulation efficiency. The method controls particle size precisely, and it also enhances the scalability and reproducibility of niosomal formulations, making it suitable for industrial applications [93].
Multiple Membrane Extrusion Method:
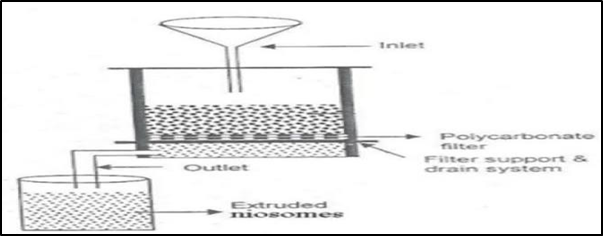
Fig No.10: Multiple Membrane Extrusion Method
The multiple membrane extrusion method of niosome production is done using a solution of surfactant, cholesterol, and dicetyl phosphate dissolved in chloroform, which is evaporated to form a thin film on the inner side of a round-bottom flask. The thin film is then hydrated with an aqueous drug solution and, while hydrating, the surfactant is converted into vesicles due to water interaction. The suspension is then extruded through polycarbonate membranes. Extrusion is generally carried out in a series of a maximum of 8 passages, which helps to reduce the niosome size and achieve homogeneity in the size distribution of the niosomes. The process is advantageous as it provides precise control of the niosome size, leading to improved reproducibility and uniformity in the final product[94].
Reverse Phase Evaporation Technique (REV):
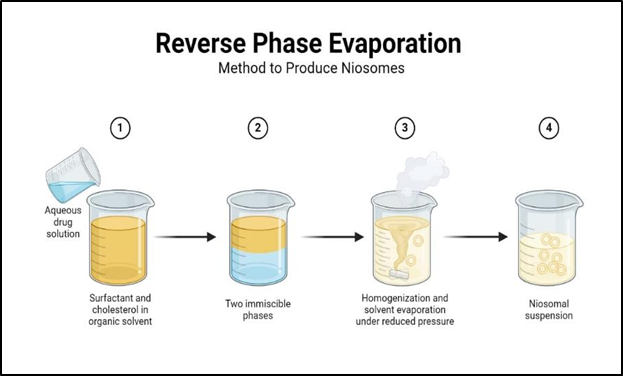
Fig No.11: Reverse Phase Evaporation Technique (REV)
In the Reverse Phase Evaporation Technique, the niosome preparation begins with dissolving the surfactant and cholesterol in a chloroform-ether mixture. An aqueous phase drug is then added to the organic phase. There are two phases afterward, and it is sonicated at low temperatures ranging from 4 to 5°C in order to make it gel-like in phase. Finally, a small volume of phosphate-buffered saline is added and sonication again is performed. The organic solvent is eliminated under low pressure at 40°C, and it forms viscous suspension of Niosomes. The suspension was then diluted in PBS and incubated at 60°C for completion of Niosomes formation [95].
Freeze-Thawing Method:
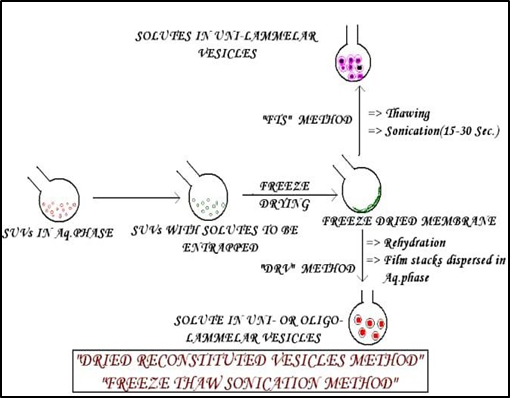
Fig No.12: Freeze-Thawing Method
The Freeze-Thawing Method for preparing niosomes involves alternating cycles of freezing and thawing the niosomal suspension. Initially, the niosomes are frozen at –20°C for a specified duration (typically 24 hours). Following this freezing period, the suspension can thaw back to ambient temperature. This process is usually repeated several times, which facilitates the fusion of niosomes and can increase vesicle diameter. The repeated freeze-thaw cycles help enhance the stability and uniformity of the niosomes. This method is appreciated for its simplicity and effectiveness in producing niosomes with desired characteristics for drug delivery applications [96].
Bubble Method:
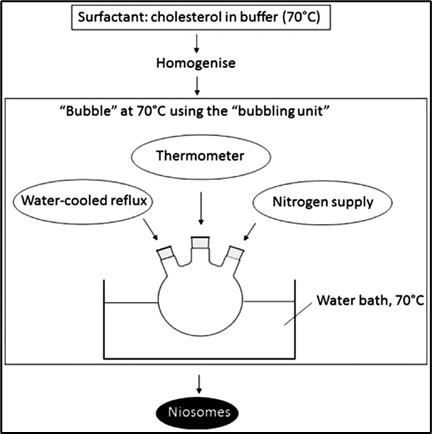
Fig No.13: Bubble Method.
The Bubble Method for preparing niosomes involves introducing air bubbles into a mixture of surfactants and cholesterol in an aqueous solution. This technique takes advantage of the aeration provided by the bubbles to facilitate the formation of niosomes. The continuous agitation and collision of bubbles create shear forces that help in the dispersion of surfactants and promote the assembly of niosomal structures. The resulting niosomes can vary in size and encapsulation efficiency, depending on the parameters such as surfactant concentration and the size of the air bubbles introduced[97].
Evaluation of Niosomes
Table No.5: Evaluation of Niosomes
|
Evaluation |
Description |
Method |
Ref |
|
Vesicle Size and Morphology |
Assessment of size distribution and shape uniformity |
Optical Microscopy, Electron Microscopy |
[98] |
|
Stability Analysis |
Monitoring physical stability, colour change, and drug retention over time at various temperatures |
UV Spectroscopy, HPLC+ |
[99] |
|
Zeta Potential Measurement |
Measurement of surface charge to assess colloidal stability and interaction with biological systems. |
Electrophoretic Light Scattering |
[100] |
|
In Vitro Drug Release Studies |
Evaluation of the rate and extent of drug release under simulated physiological conditions. |
Dialysis Tubing, Reverse Dialysis, Franz Diffusion Cell |
[101] |
|
Drug Entrapment Efficiency |
Calculation of the percentage of drug encapsulated vs. total drug amount. |
Quantitative Analysis |
[102] |
Characterization of Niosomes [103-105]
Table No.6: Characterization of Niosomes
|
Characterization Aspect |
Description |
Techniques/Methods |
|
Size Distribution |
Measurement of average size and polydispersity index (PDI). |
Dynamic Light Scattering (DLS) |
|
Morphological Analysis |
Detailed images of niosomal structures to assess morphology and internal organization. |
Transmission Electron Microscopy (TEM) |
|
Thermal Analysis |
Assessment of thermal stability and phase transitions of niosomes. |
Differential Scanning Calorimetry (DSC), Thermogravimetric Analysis (TGA) |
|
Chemical Stability |
Monitoring degradation or hydrolysis of encapsulated drugs over time. |
Stability Studies |
|
pH and Ionic Strength |
Evaluation of effects on stability and drug release profile. |
pH Studies, Ionic Strength Variations |
Applications of Niosomes [106-108]
1. Targeted Drug Delivery: Niosomes can be used for targeting drugs to specific organs, especially the reticulo-endothelial system (RES), which helps in the treatment of diseases like tumour’s and parasitic infections.
2. Anti-neoplastic Treatment: They help reduce the side effects of antineoplastic drugs by altering metabolism and prolonging circulation time, thereby enhancing the therapeutic effect.
3. Leishmaniasis Treatment: Niosomes allow higher drug levels to be administered to treat leishmaniasis without triggering significant side effects.
4. Sustained Release: They can offer sustained release of drugs, which is advantageous for drugs having low therapeutic indices and low water solubility, thereby keeping them in circulation for longer periods.
5. Localized Drug Action: Niosomes can maintain the drug at the site of administration, which is advantageous for minimally invasive treatments.
6. Adjuvant for Vaccines: Niosomes are being used to study immune responses and can function as adjuvants to enhance the efficacy of various antigens and peptides.
Challenges and Limitations
1. Stability Issues:
• Physical Instability: Niosomes tend to undergo aggregation and fusion with time, which result in changes in vesicle size and entrapment efficiency. For example, the transferosomes containing papaverine hydrochloride were found to exhibit increased size and decreased entrapment efficiency at higher storage temperatures. However, their stability was improved in the gel system over a period of 30 days at 25 °C.
• Chemical Degradation: Non-ionic surfactants used in niosome formulation are prone to oxidation and hydrolysis, which destroys the integrity of the vesicles. Studies show that niosomes are more resistant to chemical degradation or oxidation than liposomes, thus offering longer storage periods[109].
2. Drug leakage:
•Premature Release: Over time, encapsulated drugs may leak from niosomes into the gel matrix. A study on doxycycline-loaded niosomal gels reported drug leakage, leaving the free drug exposed to light and leading to degradation. This underlines the need for more stable niosomal formulations to prevent premature drug release[110].
3. Formulation Challenges:
• Complex Preparation Method: The synthesis of niosomes requires a several steps hydration, sonication, and size reduction that takes time and may also introduce variability between the batches.
• Scalability Issues: The standardization of large-scale production processes for niosomal gels is still a challenge and, therefore, not commercially applicable[111].
4. Storage and Shelf Life:
• Temperature Sensitivity: Niosomes are sensitive to temperature changes. This can have an impact on their stability. Proper storage conditions are necessary to maintain their integrity over time[112].
Future Directions:
Future research on the application of niosomal gels for rheumatoid arthritis management entails several important areas of emphasis. First, there is a requirement for better formulation methods to advance the preparation processes of niosomes, especially by investigating novel surfactants and stabilization methods to improve drug encapsulation efficiency and tailor release profiles. Moreover, extensive clinical trials are required to assess the safety, efficacy and best dosing of these formulations in clinical practice, determining their role in treatment regimens. There is also scope for personalized medicine, where niosomal gel products can be made specific to patient profiles, based on genetic or phenotypic traits of their rheumatoid arthritis. In addition, research on the efficacy of Niosomal gels as part of combination therapies may provide better therapeutic effects by treating different aspects of the disease, i.e., pain and inflammation. Thorough stability studies are required to confirm long-term efficacy of niosomal gel products, especially in temperature sensitivity and shelf life. Dried niosome precursors called proniosomes are beneficial in terms of better physical stability, storage convenience, and better penetration of the drug upon reconstitution. Their use as an alternative to traditional niosomal gels needs to be studied further, especially for transdermal and controlled drug delivery systems. Biodegradable polymers like chitosan and hyaluronic acid incorporated into proniosomal systems could also improve biocompatibility and lower the risks of toxicity. Finally, broadening the use of niosomal gels from rheumatoid arthritis to other autoimmune and inflammatory conditions will aid in measuring their ability as a drug delivery system.
CONCLUSION: Niosomal gels are a new hope in the pain management of rheumatoid arthritis (RA) by offering an efficient transdermal drug delivery system. With their novel formulation, they facilitate enhanced stability of drugs, more penetration, and localized action at target joints, hence a decrease in systemic side effects in line with traditional therapies. With ongoing research, it is important to target overcoming the stability and scalability limitations of niosomes to increase their clinical relevance. In general, niosomal gels can potentially increase patient compliance and therapeutic efficacy in the pain management of rheumatoid arthritis, leading to more specific and effective therapeutic approaches.
REFERENCES





Kavya N.*, Rashmi Mathews, Beny Baby, Tejas R., Vishal Patil, A Review On - Advances in Niosomal Gels for Management of Rheumatoid Arthritis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1548-1572 https://doi.org/10.5281/zenodo.17116003
 10.5281/zenodo.17116003
10.5281/zenodo.17116003