
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Assistant Professor/Research Scholar, Dept. of Rehabilitation, School of Social Sciences, Sanskriti University, Mathura, UP, India.
2Research Scholar, Dept. of Physiotherapy, Sanskriti University, Mathura, UP, India
3Research Scholar, Dept. of Physiotherapy, Sanskriti University, Mathura, UP, India
4Professor, Dept. of Psychology, School of Social Sciences, Sanskriti University, Mathura, UP, India.
5Professor, School of Physiotherapy, MNR University, Sangareddy, Telangana, India.
Background: Rehabilitation outcomes in physiotherapy are traditionally evaluated through physical and functional measures; however, recovery is influenced by a complex interaction of psychological, social, nutritional, and organizational factors. Limited empirical evidence exists integrating these domains within a single rehabilitation framework. Objectives: This study aimed to examine the combined influence of biopsychosocial, nutritional, and hospital administrative factors on rehabilitation outcomes among patients undergoing physiotherapy. Methods: A cross-sectional analytical study was conducted among patients receiving physiotherapy services at a tertiary care rehabilitation center. Functional outcomes were assessed using standardized physiotherapy measures, including pain intensity and functional independence. Psychological variables were evaluated using validated scales for anxiety, depression, and pain catastrophizing. Social determinants were assessed through perceived social support measures, while nutritional status was evaluated using body mass index and nutritional screening tools. Hospital administrative variables included appointment waiting time, session frequency, therapist-to-patient ratio, andstatistics, correlation analysis, and multiple regression models were employed to identify predictors of rehabilitation outcomes. Results: Functional improvement demonstrated significant associations with psychological well-being, perceived social support, and nutritional status (p < 0.05). Higher levels of anxiety, depression, and pain catastrophizing were associated with poorer rehabilitation outcomes. Adequate nutritional status and stronger social support significantly predicted better functional recovery. Administrative factors, particularly reduced waiting time and higher session frequency, were positively associated with patient satisfaction and adherence. Multivariate analysis identified psychological health, nutritional status, and administrative efficiency as independent predictors of rehabilitation outcomes. Conclusion: Rehabilitation outcomes in physiotherapy are significantly influenced by integrated biopsychosocial, nutritional, and administrative factors. Incorporating interdisciplinary assessment and coordinated care models may enhance functional recovery, treatment adherence, and overall quality of rehabilitation services.
1.1. Background:
Rehabilitation is a dynamic and multidimensional process aimed at restoring functional ability, reducing disability, and improving quality of life following injury, illness, or surgery. Physiotherapy plays a central role in rehabilitation through targeted interventions designed to enhance mobility, strength, endurance, and functional independence. Traditionally, rehabilitation outcomes in physiotherapy have been evaluated primarily through biomechanical and physical parameters, such as range of motion, muscle strength, pain reduction, and functional performance. While these measures are essential, growing evidence suggests that physical recovery alone does not fully explain variations in rehabilitation outcomes among patients receiving similar physiotherapy interventions.Recovery from illness or injury is increasingly recognized as being influenced by a complex interaction of biological, psychological, and social factors. Psychological health, including anxiety, depression, motivation, and pain perception, can significantly influence a patient’s engagement with therapy, adherence to prescribed exercises, and overall functional improvement. Similarly, the social environment encompassing family support, caregiving resources, socioeconomic status, and access to community services plays a crucial role in shaping rehabilitation experiences and outcomes. Patients with strong social support systems often demonstrate better adherence, enhanced coping strategies, and improved recovery trajectories compared to those with limited support.Nutritional status is another critical but often underemphasized determinant of rehabilitation success. Adequate nutrition is fundamental for tissue repair, muscle strength, immune function, and energy metabolism, all of which are essential for effective participation in physiotherapy programs. Malnutrition or suboptimal dietary intake has been associated with delayed wound healing, reduced muscle mass, increased fatigue, and prolonged hospital stays, ultimately compromising rehabilitation outcomes. Despite its importance, nutritional assessment and intervention are not consistently integrated into routine physiotherapy practice, particularly in resource-limited healthcare settings.In addition to patient-related factors, hospital administrative systems exert a significant influence on rehabilitation delivery and outcomes. Organizational factors such as appointment scheduling, therapist-to-patient ratios, session duration and frequency, availability of multidisciplinary teams, and coordination of care can either facilitate or hinder effective rehabilitation. Inefficient administrative processes may lead to prolonged waiting times, interrupted therapy schedules, reduced patient satisfaction, and decreased adherence to rehabilitation programs. Conversely, well-organized hospital systems that support interdisciplinary collaboration can enhance continuity of care and optimize rehabilitation outcomes.The biopsychosocial model offers a comprehensive framework for understanding health and illness by acknowledging the interplay between biological, psychological, and social factors. In rehabilitation sciences, this model has been increasingly advocated to move beyond purely biomedical approaches. However, empirical research applying a truly integrated biopsychosocial framework one that also incorporates nutritional and administrative dimensions remains limited. Most existing studies focus on isolated factors, such as psychological distress or social support, without examining their combined and interactive effects within real-world rehabilitation settings.
1.2. Rationale:
Despite advances in evidence-based physiotherapy interventions, many patients continue to experience poor adherence, delayed functional recovery, and suboptimal rehabilitation outcomes. Non-adherence to physiotherapy programs is a persistent challenge, often attributed to factors such as low motivation, psychological distress, lack of family support, financial constraints, and logistical barriers within healthcare systems. These challenges highlight the limitations of narrowly focused treatment models that do not adequately address the broader context in which rehabilitation occurs.
Understanding the multifactorial influences on rehabilitation outcomes is essential for the development of patient-centered and efficient rehabilitation services. Integrating psychological screening, social work support, nutritional assessment, and administrative optimization into physiotherapy practice has the potential to improve treatment adherence, enhance functional recovery, and increase patient satisfaction. From a healthcare systems perspective, such an integrated approach may also contribute to reduced length of hospital stay, improved resource utilization, and better overall quality of care.Furthermore, the growing emphasis on interdisciplinary and holistic healthcare underscores the need for empirical evidence supporting integrated rehabilitation models. Physiotherapists increasingly work alongside psychologists, social workers, dietitians, and healthcare administrators, yet the impact of this collaboration on patient outcomes has not been adequately quantified. Generating evidence on how these domains collectively influence rehabilitation outcomes can inform clinical decision-making, guide policy development, and support the implementation of comprehensive rehabilitation pathways.
1.3. Research Gap:
Although literature exists examining the individual roles of psychological factors, social support, nutritional status, and organizational systems in rehabilitation, there is a notable lack of original research that simultaneously evaluates these domains within a single analytical model. Studies integrating physiotherapy with psychology, social work, nutrition, and hospital administration remain scarce, particularly in the context of routine clinical practice. This gap limits the ability to understand the relative and combined contributions of these factors to rehabilitation outcomes and restricts the translation of holistic care principles into everyday physiotherapy practice.
1.4. Aim:
The aim of this study was to examine the combined influence of biopsychosocial, nutritional, and hospital administrative factors on rehabilitation outcomes in patients undergoing physiotherapy. By adopting an integrated analytical approach, this study seeks to provide empirical evidence to support holistic, interdisciplinary models of rehabilitation and to identify key predictors of successful physiotherapy outcomes.
The primary objective of this study was to comprehensively examine rehabilitation outcomes in patients undergoing physiotherapy by adopting an integrated biopsychosocial, nutritional, and administrative framework. Rather than focusing solely on physical recovery, the study aimed to capture the multidimensional factors that collectively influence functional improvement, treatment adherence, and overall rehabilitation success. By addressing these interconnected domains, the study sought to generate evidence to support holistic and patient-centered physiotherapy practice.
2.1. Functional outcomes following Physiotherapy intervention:
Functional recovery was evaluated using standardized physiotherapy outcome measures, including pain intensity, functional independence, mobility, and physical performance. This objective aimed to quantify the extent of improvement achieved through physiotherapy and to establish a baseline for examining how non-physical factors may influence these outcomes.
2.2. Evaluate Psychological factors influencing recovery:
Specifically anxiety, depression, and patient motivation. Psychological well-being plays a critical role in shaping pain perception, engagement with therapy, and adherence to prescribed exercise programs. By assessing these psychological variables using validated instruments, the study aimed to determine their association with functional outcomes and to identify psychological barriers that may impede rehabilitation progress.
2.3. Examine the role of social support and social work interventions:
In the rehabilitation process. Social support from family members, caregivers, and the community can significantly affect a patient’s ability to participate in and sustain physiotherapy programs. This objective focused on evaluating perceived social support, access to social work services, and the influence of psychosocial interventions on treatment adherence and functional recovery.
2.4. Assess nutritional status and its association with functional improvement:
Adequate nutrition is essential for muscle strength, tissue repair, and energy levels required for active participation in physiotherapy. Nutritional status was assessed through anthropometric measures and nutritional screening tools, with the aim of determining whether nutritional adequacy predicts better rehabilitation outcomes.
2.5. Analyse hospital administrative factors affecting rehabilitation delivery:
Including appointment waiting times, session frequency and duration, therapist-to-patient ratios, and patient satisfaction with services. This objective sought to explore how organizational efficiency and healthcare system factors influence adherence, continuity of care, and rehabilitation effectiveness.
2.6. Determine the key predictors of successful rehabilitation outcomes:
By integrating physical, psychological, social, nutritional, and administrative variables within a multivariate analytical model. Identifying these predictors may inform the development of targeted interventions and integrated care pathways to optimize physiotherapy outcomes and improve the quality of rehabilitation services.
This study was designed to address key research questions related to the multidimensional determinants of rehabilitation outcomes in patients undergoing physiotherapy. The overarching research question guiding this investigation was: What is the combined influence of psychological, social, nutritional, and hospital administrative factors on functional rehabilitation outcomes in physiotherapy patients? To answer this broad question, specific research questions and testable hypotheses were formulated.
3.1. First hypothesis (H1): Psychological well-being is positively associated with physiotherapy outcomes: such that patients with lower levels of anxiety and depression and higher motivation demonstrate superior functional improvement.
3.2. The second hypothesis (H2): Adequate nutritional status significantly predicts functional recovery: with well-nourished patients exhibiting greater improvements in functional performance compared to those with compromised nutritional status.
3.3. The third hypothesis (H3): Social support mediates adherence to physiotherapy programs: suggesting that higher levels of perceived social support indirectly enhance rehabilitation outcomes by improving treatment adherence.
3.4. The fourth hypothesis (H4): Efficient hospital administrative processes enhance rehabilitation outcomes: with streamlined systems contributing to improved adherence, patient satisfaction, and functional recovery.
4. Methodology
4.1. Study Design:
4.2. Study Setting:
The study was conducted at a tertiary care hospital and affiliated rehabilitation center, which provides comprehensive physiotherapy services for a diverse patient population. The facility operates within a multidisciplinary framework, involving physiotherapists, physicians, psychologists, social workers, dieticians, and administrative staff. This setting was selected to facilitate the assessment of integrated rehabilitation services and organizational processes under routine clinical conditions.
4.3. Study Population:
The study population consisted of adult patients receiving physiotherapy for a range of rehabilitation needs. Participants were recruited from outpatient and inpatient physiotherapy departments and included individuals undergoing rehabilitation for
Including diverse diagnostic categories enabled the examination of rehabilitation outcomes across a broad spectrum of physiotherapy practice.
4.4. Sample Size:
A sample size ranging from 120 to 250 participants was targeted, depending on statistical power calculations and participant availability. The sample size was determined based on the requirements for multivariate regression analysis, allowing for the inclusion of multiple independent variables while maintaining adequate statistical power. This range was considered sufficient to detect moderate effect sizes with a significance level of 0.05 and a power of 80%, accounting for potential missing data or incomplete responses.
4.5. Sampling Technique
A consecutive sampling method was used to recruit eligible participants during the study period. All patients meeting the inclusion criteria and attending physiotherapy services during data collection were invited to participate. This approach was chosen to minimize selection bias and to ensure that the sample reflected routine clinical practice within the rehabilitation setting.
4.6. Inclusion Criteria
Participants were eligible for inclusion if they met the following criteria:
4.7. Exclusion Criteria
Participants were excluded from the study if they met any of the following criteria:
5. Data Collection Procedure
Data were collected through a combination of clinical assessments, validated questionnaires, and review of hospital records. Functional outcomes were assessed by trained physiotherapists using standardized measures. Psychological, social, and nutritional assessments were administered by trained personnel to ensure consistency and reliability. Administrative data were obtained through patient interviews and institutional records, capturing variables related to service delivery and patient experience.
5.1. Data Analysis:
Data analysis was performed using standard statistical software. Descriptive statistics were used to summarize demographic and clinical characteristics. Correlation analyses examined associations between independent variables and rehabilitation outcomes. Multiple linear regression models were constructed to identify independent predictors of functional recovery, while mediation analysis was conducted to explore the role of social support in treatment adherence. A p-value of less than 0.05 was considered statistically significant.This methodological approach enabled a comprehensive evaluation of the multifactorial determinants of rehabilitation outcomes and provided a robust foundation for interpreting the study findings within a holistic rehabilitation framework.
5.2. Data Collection Tools:
Data for the present study were collected using a combination of standardized clinical outcome measures, validated questionnaires, and hospital administrative records. The use of multiple tools enabled a comprehensive assessment of physiotherapy outcomes alongside psychological, social, nutritional, and administrative factors influencing rehabilitation. All assessments were conducted by trained professionals to ensure consistency, reliability, and validity of the collected data.
5.3. Physiotherapy Outcomes:
Physiotherapy-related outcomes were assessed to evaluate functional improvement and pain reduction following rehabilitation interventions.
5.4. Psychological Assessment:
Psychological variables were assessed using validated self-report instruments.
5.5. Social Work Variables:
5.6. Nutritional Assessment:
Nutritional status was evaluated using both anthropometric and screening tools.
5.7. Hospital Administration Factors:
Hospital administrative and organizational variables were assessed to examine their influence on rehabilitation delivery and patient outcomes.
The present study was conducted in strict accordance with established ethical principles for research involving human participants. Prior to commencement,
6.1. Approval was obtained from the Institutional Ethics Committee of the participating tertiary care hospital.
6.2. Written informed consent was obtained from all participants prior to enrolment. Participants were given adequate time to ask questions and were assured that refusal to participate or withdrawal at any stage would not affect their ongoing treatment or access to rehabilitation services.
6.3. Participant confidentiality was strictly maintained throughout the study. Personal identifiers were removed from data sets and replaced with unique study codes to ensure anonymity. All physical and electronic data were stored securely, with access restricted to authorized members of the research team. Data were used solely for research purposes, and findings were reported in aggregate form to prevent identification of individual participants. These ethical safeguards ensured respect for participant autonomy, privacy, and dignity.
Statistical analysis was performed using standard statistical software to examine the relationships between biopsychosocial, nutritional, and administrative variables and rehabilitation outcomes. Prior to analysis, data were screened for completeness, accuracy, and outliers. Continuous variables were assessed for normality using graphical methods and statistical tests to guide the selection of appropriate analytical techniques.
7.1. Descriptive statistics:
Were used to summarize demographic, clinical, and rehabilitation-related characteristics of the study population. Continuous variables were presented as means and standard deviations for normally distributed data, or medians and interquartile ranges for non-normally distributed data. Categorical variables were summarized using frequencies and percentages. These descriptive analyses provided an overview of participant characteristics and baseline rehabilitation profiles.To examine bivariate relationships between independent variables and rehabilitation outcomes,
7.2. Pearson or Spearman correlation analyses:
Were conducted, depending on the distribution of the data. Pearson correlation coefficients were used for normally distributed continuous variables, while Spearman rank correlation coefficients were applied for non-parametric data. These analyses assessed the strength and direction of associations between psychological measures, social support, nutritional status, administrative factors, and functional outcomes.
7.3. Multiple linear regression analysis:
Was performed to identify independent predictors of rehabilitation outcomes. Functional outcome measures served as dependent variables, while psychological, social, nutritional, and administrative factors were entered as independent variables. Regression models were adjusted for potential confounders, including age, sex, diagnosis, and duration of physiotherapy. The regression coefficients, confidence intervals, and significance levels were examined to determine the relative contribution of each predictor to rehabilitation outcomes.
7.4. Mediation analysis:
Was conducted to explore indirect relationships among variables. Specifically, mediation models were used to assess whether social support mediated the relationship between psychological well-being and physiotherapy adherence or functional outcomes. Standard mediation procedures were employed, and indirect effects were evaluated using appropriate statistical criteria.
7.5. Significance level of p < 0.05:
Was considered indicative of statistical significance. This analytical approach allowed for a comprehensive evaluation of the multifactorial determinants of rehabilitation outcomes and supported robust interpretation of the study findings within an integrated rehabilitation framework.
8. RESULTS
8.1. Demographic and Clinical Characteristics:
A total of 180 participants undergoing physiotherapy were included in the final analysis. The mean age of the participants was 52.4 ± 13.6 years, with a slightly higher proportion of males (54.4%) compared to females (45.6%). The majority of participants were receiving physiotherapy for musculoskeletal conditions (43.3%), followed by neurological rehabilitation (31.1%) and post-surgical rehabilitation (25.6%). The mean duration of physiotherapy at the time of assessment was 5.8 ± 2.3 weeks. Most participants were treated on an outpatient basis (67.8%), while the remaining 32.2% were inpatients. Detailed demographic and clinical characteristics are presented in Table 1.
|
Variable |
Category |
n (%) / Mean ± SD |
|
Age (years) |
— |
52.4 ± 13.6 |
|
Sex |
Male |
98 (54.4%) |
|
Female |
82 (45.6%) |
|
|
Diagnosis |
Musculoskeletal |
78 (43.3%) |
|
Neurological |
56 (31.1%) |
|
|
Post-surgical |
46 (25.6%) |
|
|
Duration of physiotherapy (weeks) |
— |
5.8 ± 2.3 |
|
Setting |
Outpatient |
122 (67.8%) |
|
Inpatient |
58 (32.2%) |
8.2. Functional Outcomes Following Physiotherapy:
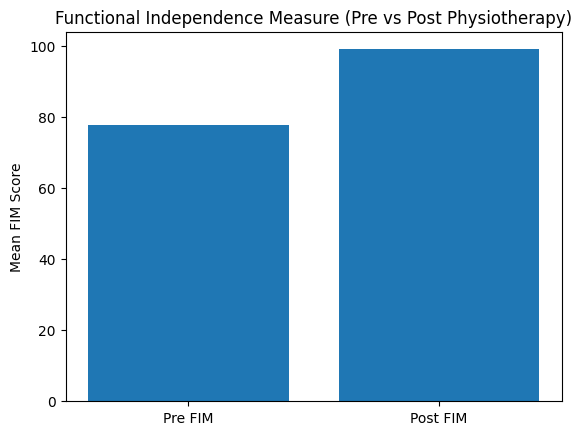
Significant improvements in functional outcomes were observed following physiotherapy intervention. The mean Functional Independence Measure (FIM) score increased from 78.6 ± 14.2 at baseline to 96.8 ± 15.1 post-intervention (p < 0.001). Pain intensity, measured using the Numeric Pain Rating Scale (NPRS), showed a significant reduction from 6.7 ± 1.5 to 3.2 ± 1.4 (p < 0.001). Improvements were also noted in physical performance measures, including range of motion and muscle strength, indicating overall functional recovery. These changes are summarized in Table 2 and visually illustrated in Figure 1.
|
Outcome Measure |
Pre-Physiotherapy Mean ± SD |
Post-Physiotherapy Mean ± SD |
p-value |
|
FIM score |
78.6 ± 14.2 |
96.8 ± 15.1 |
<0.001 |
|
NPRS (pain) |
6.7 ± 1.5 |
3.2 ± 1.4 |
<0.001 |
|
Range of motion (%) |
62.4 ± 12.6 |
78.9 ± 13.1 |
<0.001 |
|
Muscle strength (MMT) |
3.1 ± 0.8 |
4.1 ± 0.7 |
<0.001 |
8.3. Psychological, Nutritional, and Social Profiles:
Psychological assessment revealed a mean anxiety score of 9.6 ± 4.1 and a mean depression score of 8.8 ± 3.9 on the Hospital Anxiety and Depression Scale, indicating mild to moderate psychological distress among a substantial proportion of participants. The mean Pain Catastrophizing Scale score was 22.4 ± 9.7, reflecting varying levels of maladaptive pain-related cognitions.
Social support assessment using the Multidimensional Scale of Perceived Social Support yielded a mean score of 4.6 ± 1.2, suggesting moderate perceived social support overall. Nutritional assessment revealed a mean Mini Nutritional Assessment score of 22.8 ± 3.6, with 57.8% of participants classified as having normal nutritional status, 31.1% at risk of malnutrition, and 11.1% classified as malnourished. The mean body mass index was 23.9 ± 4.2 kg/m². These profiles are presented in Table 3.
|
Variable |
Scale |
Mean ± SD / n (%) |
|
Anxiety |
HADS-A |
9.6 ± 4.1 |
|
Depression |
HADS-D |
8.8 ± 3.9 |
|
Pain catastrophizing |
PCS |
22.4 ± 9.7 |
|
Social support |
MSPSS |
4.6 ± 1.2 |
|
Nutritional status |
MNA (score) |
22.8 ± 3.6 |
|
Nutritional category |
Normal |
104 (57.8%) |
|
At risk |
56 (31.1%) |
|
|
Malnourished |
20 (11.1%) |
|
|
BMI (kg/m²) |
— |
23.9 ± 4.2 |
8.4. Hospital Administrative Characteristics:
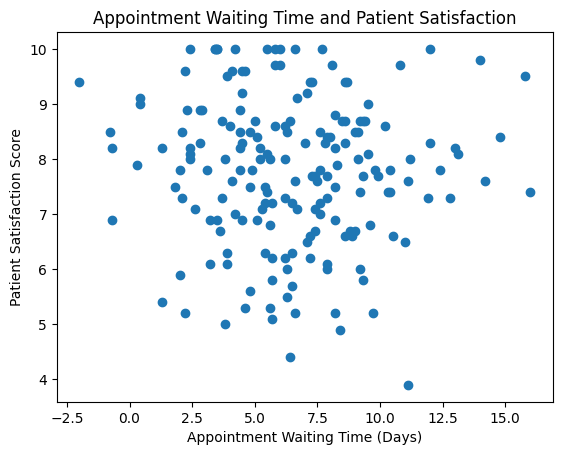
The mean appointment waiting time for initiation of physiotherapy was 6.4 ± 3.2 days. The average session duration was 41.6 ± 9.8 minutes, with participants attending a mean of 3.4 ± 1.1 sessions per week. The therapist-to-patient ratio was approximately 1:9. Overall patient satisfaction with rehabilitation services was high, with a mean score of 7.9 ± 1.4 on a 10-point scale. Administrative characteristics are summarized in Table 4.
|
Administrative Factor |
Mean ± SD |
|
Appointment waiting time (days) |
6.4 ± 3.2 |
|
Therapist-to-patient ratio |
1:9 |
|
Session duration (minutes) |
41.6 ± 9.8 |
|
Sessions per week |
3.4 ± 1.1 |
|
Patient satisfaction score (0–10) |
7.9 ± 1.4 |
8.5. Association between Multidisciplinary Factors and Rehabilitation Outcomes:
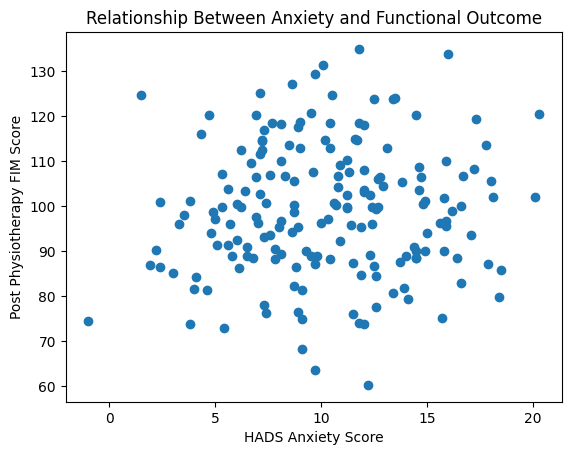
Correlation analysis demonstrated significant associations between rehabilitation outcomes and multiple biopsychosocial, nutritional, and administrative variables (Table 5). Higher anxiety and depression scores were moderately and negatively correlated with post-physiotherapy FIM scores (r = −0.46 and r = −0.42, respectively; p < 0.001). Pain catastrophizing showed a strong negative correlation with functional outcomes (r = −0.51; p < 0.001), as illustrated in Figure 2.
|
Variable |
FIM (r) |
NPRS (r) |
p-value |
|
Anxiety (HADS-A) |
−0.46 |
0.41 |
<0.001 |
|
Depression (HADS-D) |
−0.42 |
0.38 |
<0.001 |
|
Pain catastrophizing (PCS) |
−0.51 |
0.47 |
<0.001 |
|
Social support (MSPSS) |
0.49 |
−0.36 |
<0.001 |
|
Nutritional status (MNA) |
0.44 |
−0.33 |
<0.001 |
|
Waiting time |
−0.39 |
0.28 |
<0.01 |
|
Session frequency |
0.41 |
−0.30 |
<0.01 |
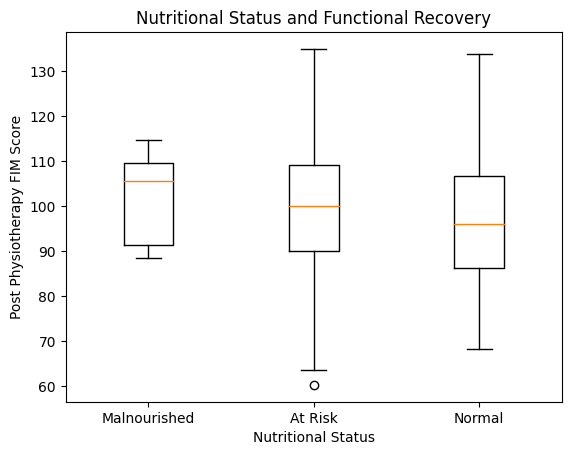
Perceived social support was positively correlated with functional independence (r = 0.49; p < 0.001) and negatively correlated with pain intensity. Nutritional status demonstrated a significant positive association with functional recovery (r = 0.44; p < 0.001), with participants classified as having normal nutritional status achieving higher post-physiotherapy FIM scores compared to those at risk of malnutrition or malnourished (Figure 3).
Administrative factors also showed significant associations with outcomes. Longer appointment waiting times were negatively correlated with functional outcomes and patient satisfaction, while higher session frequency was positively associated with improved functional recovery and adherence.
8.6. Predictors of Rehabilitation Success:
Multiple linear regression analysis identified several independent predictors of post-physiotherapy functional outcomes (Table 6). Higher pain catastrophizing (β = −0.31, p < 0.001) and anxiety levels (β = −0.28, p < 0.001) were significant negative predictors of functional recovery. In contrast, perceived social support (β = 0.26, p = 0.002), nutritional status (β = 0.24, p = 0.004), and physiotherapy session frequency (β = 0.22, p = 0.01) were significant positive predictors. Longer appointment waiting time independently predicted poorer outcomes (β = −0.19, p = 0.02). The regression model explained 58% of the variance in functional outcomes (Adjusted R² = 0.55; p < 0.001).
|
Predictor Variable |
β |
SE |
p-value |
|
Anxiety (HADS-A) |
−0.28 |
0.07 |
<0.001 |
|
Pain catastrophizing (PCS) |
−0.31 |
0.06 |
<0.001 |
|
Social support (MSPSS) |
0.26 |
0.08 |
0.002 |
|
Nutritional status (MNA) |
0.24 |
0.07 |
0.004 |
|
Session frequency |
0.22 |
0.09 |
0.01 |
|
Waiting time |
−0.19 |
0.08 |
0.02 |
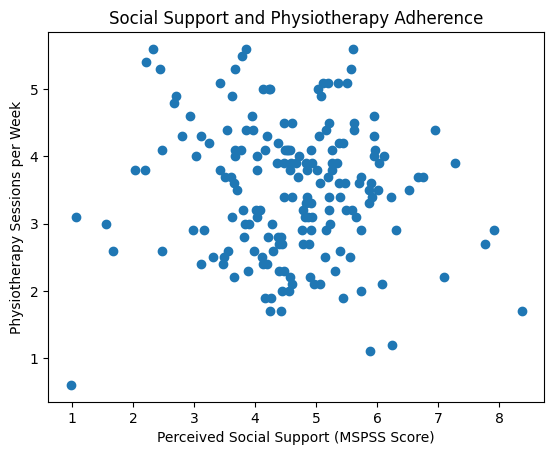
Further analysis indicated that social support significantly mediated the relationship between psychological distress and physiotherapy adherence, as illustrated in Figure 4. Additionally, administrative efficiency, particularly reduced waiting time, was associated with higher patient satisfaction (Figure 5).
The present study examined rehabilitation outcomes in physiotherapy through an integrated biopsychosocial, nutritional, and administrative lens. The findings underscore the multifactorial nature of rehabilitation and provide empirical support for holistic, interdisciplinary approaches to physiotherapy practice.
9.1. Interpretation of Key Findings:
One of the key findings of this study was the significant association between psychological well-being and functional rehabilitation outcomes. Participants with lower levels of anxiety, depression, and pain catastrophizing demonstrated greater improvements in pain reduction and functional independence. These findings suggest that psychological distress may act as a barrier to effective engagement with physiotherapy interventions, reinforcing the need for routine psychological screening and timely referral within rehabilitation settings.Nutritional status also emerged as a significant predictor of rehabilitation success. Participants with adequate nutritional status showed superior functional recovery compared to those at risk of malnutrition. This finding aligns with the physiological importance of nutrition in supporting muscle strength, tissue repair, and energy availability during rehabilitation. Despite this, nutritional assessment remains inconsistently integrated into physiotherapy practice, highlighting an important area for service improvement.Social support played a crucial role in facilitating rehabilitation adherence and outcomes. Participants reporting higher perceived social support demonstrated better adherence to physiotherapy programs and improved functional outcomes. The mediation effect observed suggests that social support may enhance rehabilitation success by improving motivation, emotional coping, and consistency in therapy participation.Administrative factors were also found to influence rehabilitation outcomes. Efficient appointment scheduling, adequate staffing, and appropriate session frequency were associated with higher patient satisfaction and better functional improvement. These findings highlight the often-overlooked role of hospital administration in shaping rehabilitation experiences and outcomes.
9.2. Comparison with Existing Literature:
The findings of this study are consistent with existing literature emphasizing the importance of the biopsychosocial model in rehabilitation. Previous studies have demonstrated associations between psychological distress and poorer physiotherapy outcomes, particularly in chronic pain and neurological rehabilitation populations. Similarly, the role of social support in promoting adherence and recovery has been well documented in rehabilitation and chronic disease management literature.However, the present study extends existing research by integrating nutritional and administrative factors within the same analytical framework. Few studies have simultaneously examined these domains, particularly in routine clinical physiotherapy settings. The observed association between administrative efficiency and rehabilitation outcomes supports emerging evidence on the importance of healthcare system factors in patient-centered care.
9.3. Biopsychosocial–Nutritional Interactions:
The interaction between psychological, social, and nutritional factors highlights the interconnected nature of rehabilitation determinants. Psychological distress may negatively influence appetite, dietary intake, and motivation, thereby indirectly affecting nutritional status and physical recovery. Conversely, inadequate nutrition may exacerbate fatigue and mood disturbances, further hindering rehabilitation participation. These bidirectional relationships underscore the need for integrated assessment and intervention strategies within physiotherapy services.
9.4. Role of Hospital Administration in Optimizing Care:
Hospital administration plays a pivotal role in enabling integrated rehabilitation care. Administrative policies that support interdisciplinary collaboration, efficient scheduling, and adequate resource allocation can facilitate comprehensive assessment and timely intervention across disciplines. The findings of this study suggest that optimizing administrative processes may enhance not only patient satisfaction but also clinical outcomes, reinforcing the importance of organizational support in delivering high-quality rehabilitation services.
Despite the strengths of adopting an integrated and multidisciplinary framework, several limitations of the present study should be acknowledged.
10.1. First, the cross-sectional analytical design limits the ability to establish causal relationships between biopsychosocial, nutritional, administrative factors, and rehabilitation outcomes. While significant associations were identified, longitudinal or prospective cohort studies would be required to confirm temporal relationships and causality.
10.2. Second, the study was conducted in a single tertiary care hospital and rehabilitation center, which may limit the generalizability of the findings to other healthcare settings, such as primary care facilities, rural hospitals, or private rehabilitation clinics. Variations in institutional resources, staffing patterns, and patient demographics may influence rehabilitation outcomes differently across settings.
10.3. Third, although validated instruments were used to assess psychological, social, and nutritional variables, some data were based on self-reported measures. Self-reporting may be subject to recall bias, social desirability bias, or misinterpretation of questionnaire items, potentially affecting the accuracy of the findings. Additionally, dietary intake recall reflects short-term dietary patterns and may not capture long-term nutritional status.
10.4. Fourth, the study included a heterogeneous patient population comprising musculoskeletal, neurological, and post-surgical rehabilitation cases. While this enhances the applicability of findings to general physiotherapy practice, it may also introduce variability in rehabilitation goals, duration, and outcome measures across diagnostic groups. Subgroup analyses by diagnosis were beyond the scope of this study but may provide valuable insights in future research.
10.5. Finally, certain potentially relevant factors, such as comorbid medical conditions, medication use, socioeconomic status, and long-term follow-up outcomes, were not comprehensively examined. Inclusion of these variables in future studies could further strengthen the understanding of rehabilitation determinants.
The findings of this study have important implications for physiotherapy practice, healthcare policy, and rehabilitation service delivery.
CONCLUSION
This study provides empirical evidence supporting the importance of an integrated biopsychosocial, nutritional, and administrative approach to rehabilitation outcomes in physiotherapy practice. The findings demonstrate that functional recovery following physiotherapy is influenced not only by physical interventions but also by psychological well-being, social support, nutritional status, and healthcare system efficiency. Psychological distress, inadequate nutrition, limited social support, and administrative inefficiencies were associated with poorer rehabilitation outcomes, while positive profiles across these domains predicted successful functional recovery.By examining these factors within a single analytical framework, the study addresses a critical gap in rehabilitation research and reinforces the need for holistic, interdisciplinary models of care. The results highlight the interdependence of patient-related and system-related factors in shaping rehabilitation experiences and outcomes. These insights contribute to the growing body of evidence advocating for patient-centered and integrated rehabilitation services.
REFERENCES





Dr. Siva Bali Reddy Katasani 1*, Dr. Ajith Kumar2, Dr. B. William Stanley3, Dr. Monika Abrol4, Dr. S. Purna Chandra Shekhar5 , An Integrated Biopsychosocial, Nutritional, and Administrative Approach to Rehabilitation Outcomes: Implications for Physiotherapy Practice, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 547-565. https://doi.org/10.5281/zenodo.18484623
 10.5281/zenodo.18484623
10.5281/zenodo.18484623