
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Godavari Institute of Pharmacy Kolpa, Latur- 413512, Maharashtra, India.
Is a rare but life-threatening fungal infection caused by fungi belonging to the order Mucorales, predominantly Rhizopus, Mucor, Rhizomucor, and Lichtheimia. The infection is characterized by rapid tissue necrosis and has a high mortality rate if not diagnosed and treated promptly. Mucormycosis primarily affects immunocompromised individuals, including those with uncontrolled diabetes mellitus, hematological malignancies, solid organ transplants, and those undergoing prolonged corticosteroid therapy. The disease typically manifests in four clinical forms: rhino-orbital-cerebral, pulmonary, gastrointestinal, and cutaneous. Rhino-orbital-cerebral mucormycosis is the most common and is often associated with diabetic ketoacidosis, where the fungus invades the sinuses, spreading to the orbit and brain. Early diagnosis relies on clinical suspicion, radiological imaging, histopathological examination, and microbiological cultures. Treatment involves a combination of antifungal therapy, usually with liposomal amphotericin B, and, when feasible, surgical debridement of necrotic tissue. Despite aggressive treatment, the prognosis remains poor, particularly in patients with extensive disease or underlying immunocompromise. Preventive strategies focus on controlling predisposing factors, such as optimal management of diabetes and minimizing the use of immunosuppressive agents. The increasing incidence of mucormycosis, particularly in the context of the COVID-19 pandemic, highlights the need for greater awareness, early detection, and timely intervention. This review article presents the current statistics, the causes of this infection in the human body, and its diagnosis with available recent therapies through recent databases collected from several clinics and agencies. The diagnosis and identifcation of the infection were made possible through various latest medical techniques such as computed tomography scans, direct microscopic observations, MALDI-TOF mass spectrometry, serology, molecular assay, and histopathology.
Mucormycosis, also known as zygomycosis, is a rare but serious fungal infection caused by a group of molds known as mucormycetes. These fungi are typically found in decaying organic matter such as soil, leaves, compost, and decaying fruit. When the spores of these molds are inhaled or come into contact with broken skin, they can lead to severe infections, particularly in individuals with compromised immune systems. Mucormycosis predominantly affects people who are immunocompromised, such as those with uncontrolled diabetes, cancer, organ transplants, or those taking immunosuppressive medications. It can also affect individuals with severe trauma or burns, or those with chronic conditions like kidney failure.
The infection can manifest in several different forms, depending on the area of the body that is affected:
Symptoms of mucormycosis can vary based on the site of infection but may include fever, headache, facial swelling, black lesions (especially in the nose or mouth), chest pain, difficulty breathing, and gastrointestinal discomfort. Because of its rapid progression and the need for immediate treatment, mucormycosis is considered a medical emergency.
Underlying conditions associated with mucormycosis:
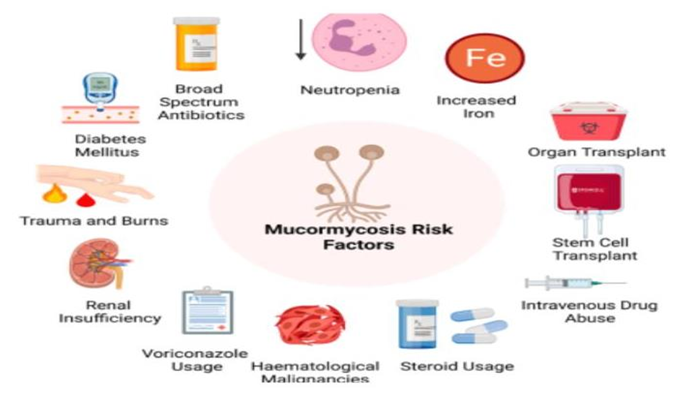
Mucormycosis has been associated with various underlying conditions that predispose an individual to the infection. Some of these factors include diabetes, neutropenia, organ or stem cell transplantation, trauma and burns, hematological disorders, steroidal use, metabolic acidosis, intravenous drug usage, renal insufficiency, broad-spectrum antibiotics, increase in iron in the system, malnutrition, usage of voriconazole (Fig. 2) (Dantas et al., 2021; Sarvestani et al., 2013; Shariati et al., 2020; Suganya et al., 2019). A previous study from Europe (Skiada et al., 2011) showed that, the most significant underlying causes were hematological malignancies, while it was diabetes mellitus in India (Chakrabarti et al., 2009), Iran (Dolatabadi et al., 2018), Middle East, North Africa (Stemler et al., 2020) and Mexico (Corzo-Leon ´ et al., 2018). Among the different forms of mucormycosis, ROCM has been concomitant with the presence of diabetes. The cutaneous form was more prominent in individuals with trauma, and organ transplant was related to the pulmonary, gastrointestinal and disseminated type. In addition, underlying hematological malignancies were present in disseminated type and neutropenia in the pulmonary form (Jeong et al., 2019). Mucormycosis occurs mainly in individuals with uncontrolled diabetes, and this is because the innate immunity in these individuals, impacts the polymorphonuclear phagocytes to destroy the fungi. In patients with diabetes, the sinus was the most affected area followed by the pulmonary areas (Rammaert et al., 2012). Individuals with hematological malignancies were also predisposed to mucormycosis during the neutropenia phase of the ailment.
Classification of mucormycosis
Mucormycosis, also known as zygomycosis, is a rare but serious fungal infection caused by molds in the order Mucorales. The classification of mucormycosis can be understood from both a clinical and a microbiological perspective. Below is a breakdown of the classification based on these two frameworks:
1. Clinical Classification of Mucormycosis
Mucormycosis can affect various parts of the body, leading to different clinical presentations. Based on the site of infection, mucormycosis is classified into the following types: a. Rhinocerebral Mucormycosis
b. Pulmonary Mucormycosis
Cutaneous Mucormycosis
Renal Mucormycosis
Disseminated Mucormycosis
2. Microbiological Classification (Fungal Taxonomy)
The causative organisms of mucormycosis belong to the Mucorales order, within the class Zygomycetes. The major genera that cause mucormycosis include: a. Rhizopus
Lichtheimia (formerly Absidia)
? Species such as Lichtheimia corymbifera are important pathogens in mucormycosis. d. Cunninghamella
? Less common but still implicated in infections, especially in immunocompromised patients.
Syncephalastrum
? Occasionally causes mucormycosis, particularly in patients with hematologic malignancies or those undergoing organ transplantation.

Fig.1 Structures of Rhizopus
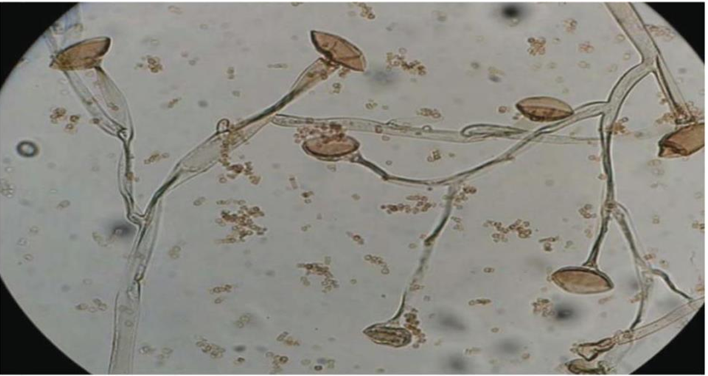
Fig.2 Structure of Rhizopus
3. Risk Factors for Mucormycosis
Mucormycosis predominantly affects immunocompromised individuals. Common risk factors include:
4. Diagnostic Classification
Diagnosis of mucormycosis typically involves a combination of clinical, microbiological, and imaging studies:
5. Treatment Classification
Treatment generally involves a combination of: ? Surgical debridement of necrotic tissue.
Sign and Symptom
The signs and symptoms of mucormycosis vary depending on the site of infection, the underlying health conditions of the patient, and the severity of the disease. Mucormycosis can affect different parts of the body, including the sinuses, lungs, skin, gastrointestinal tract, and brain. Below is an overview of the typical signs and symptoms of mucormycosis based on the affected organ/system:
1. Rhinocerebral Mucormycosis
This is the most common form of mucormycosis, primarily affecting the sinuses and brain. It is often seen in diabetic patients (especially those with diabetic ketoacidosis) and immunocompromised individuals.
Signs and Symptoms:
Nasal congestion and discharge (often purulent or bloody).
2. Pulmonary Mucormycosis
This form affects the lungs and is typically seen in patients with conditions such as hematological malignancies, organ transplant recipients, neutropenic patients, and those receiving immunosuppressive therapy.
Signs and Symptoms:
3. Gastrointestinal Mucormycosis
Involvement of the gastrointestinal (GI) tract is rare but can be seen, particularly in neonates, premature infants, and severely immunocompromised individuals.
Signs and Symptoms:
4. Cutaneous Mucormycosis
Cutaneous mucormycosis typically results from direct inoculation of spores through trauma, surgery, or burns. It is often seen in diabetic patients or those with skin wounds.
Signs and Symptoms:
5. Renal Mucormycosis
Though rare, mucormycosis can also involve the kidneys, particularly in patients with diabetes, chronic kidney disease, or those on dialysis.
Signs and Symptoms:
Risk factors: -
The development of mucormycosis is closely linked to several risk factors that primarily involve immune suppression and disruption of normal host defenses. These factors make individuals more susceptible to the fungal infection by impairing their ability to prevent fungal spores (conidia) from invading tissues and causing disease. Below are the key risk factors for mucormycosis:
1. Diabetes Mellitus
Diabetes, especially in patients with poorly controlled blood sugar levels or diabetic ketoacidosis (DKA), is one of the most significant risk factors for mucormycosis.
2. Immunocompromised States
This includes individuals with:
3. Corticosteroid Use
4. Neutropenia
5. Chronic Kidney Disease (CKD) and Dialysis
6. Trauma, Burns, and Surgical Wounds
7. Prematurity and Neonatal Conditions
8. High Iron Levels (Iron Overload)
9. Cancer (Especially Hematologic Malignancies)
10. Malnutrition
Pathophysiology:
The pathophysiology of mucormycosis involves a complex interplay between the Mucorales fungi, the host's immune response, and various predisposing factors. These fungi, including species like Rhizopus, Mucor, Lichtheimia, and others, are typically opportunistic pathogens that cause infections primarily in individuals with immunocompromised states or underlying conditions. The pathogenesis is driven by the inhalation of fungal spores (conidia), their germination, and subsequent invasive growth, leading to tissue necrosis, dissemination, and potentially systemic infection.
Overview of Key Steps in Pathophysiology
1. Entry and Germination of Spores
2. Angioinvasion
3. Immune Evasion
4. Tissue Necrosis and Inflammation
5. Dissemination and Systemic Infection
6. Clinical Manifestations
As the infection becomes more invasive, symptoms worsen rapidly, including:
Diagnosis
The diagnosis of mucormycosis is a challenging process that requires a high index of suspicion, especially since the disease can progress rapidly and may be mistaken for other conditions. A combination of clinical evaluation, microbiological testing, and imaging studies is essential for accurate diagnosis. Early identification and treatment are crucial for improving outcomes, as mucormycosis has a high mortality rate if not treated promptly.
Here’s a detailed look at the steps involved in diagnosing mucormycosis:
1. Clinical Suspicion
The diagnosis of mucormycosis begins with clinical suspicion, based on symptoms, patient history, and risk factors. Key clues include:
2. Microbiological Diagnosis
Once mucormycosis is suspected, microbiological testing plays a critical role in confirming the diagnosis.
A. Direct Microscopic Examination
B. Histopathological Examination
Biopsy specimens (e.g., skin, sinuses, lung tissue) are often collected for histological examination.
C. Fungal Culture
D. Polymerase Chain Reaction (PCR)
E. Serologic Testing
3. Imaging Studies
Imaging plays a key role in identifying the extent of infection, guiding biopsy procedures, and assessing complications like vascular invasion and tissue necrosis.
A. CT Scan (Computed Tomography)
B. MRI
C. Angiography (for Disseminated Disease)
- Angiography (e.g., CT angiography or MRI angiography) may be used to assess vascular involvement or thrombosis caused by fungal invasion, particularly in disseminated mucormycosis.
4. Blood Tests
While blood cultures for Mucorales are typically negative, some blood tests may offer supportive information or help in monitoring the disease:
Treatments
The treatment of mucormycosis requires a multidisciplinary approach involving antifungal therapy, surgical intervention, and addressing underlying risk factors. Mucormycosis is a rapidly progressing and often life-threatening infection, so prompt treatment is essential for improving outcomes. The overall approach to treatment is typically divided into the following components:
1. Antifungal Therapy
The cornerstone of medical management of mucormycosis is the use of antifungal medications. Treatment often needs to be initiated empirically while awaiting the results of microbiological testing, and the choice of antifungal agent is based on fungal species and severity of infection.
A. First-line Antifungal Agents
Amphotericin B is the first-line antifungal treatment for mucormycosis.
B. Other Amphotericin B Formulations
- Conventional amphotericin B is sometimes used if liposomal amphotericin is not available, but it has a higher risk of nephrotoxicity and infusion-related reactions. Dosage is typically 0.5–1 mg/kg/day intravenously.
C. Posaconazole
D. Isavuconazole
E. Combination Therapy
- In severe cases, combination therapy with both amphotericin B and posaconazole or isavuconazole may be considered, though the evidence for improved outcomes with combination therapy is still limited.
F. Emerging Therapies
- Echinocandins (e.g., caspofungin, micafungin) have limited activity against Mucorales, but they are sometimes considered in refractory cases or as part of combination therapy. However, their efficacy is not as well established as that of amphotericin B.
2. Surgical Treatment
Surgical debridement is critical in the management of mucormycosis, especially for infections in sinuses, skin, or lungs. Fungus is often deeply embedded in tissues, and antifungal therapy alone is insufficient for controlling the infection.
A. Necrotic Tissue Debridement
B. Amputation (for severe cases)
- In cases of extensive tissue necrosis (e.g., in patients with diabetic foot infections), amputation of the affected limb may be required to save the patient’s life.
C. Orbital Decompression
- In orbital mucormycosis with involvement of the eye, orbital decompression surgery may be necessary to remove infected tissue, including the orbital contents (e.g., eyeball) in severe cases.
3. Management of Underlying Conditions
Managing underlying risk factors is a key aspect of treatment. Correction of the predisposing factors can help improve the patient’s immune response and reduce the risk of further fungal infections.
A. Diabetes Management
B. Immunosuppressive Therapy
- For patients with a history of organ transplantation or hematologic malignancies, reducing or modifying immunosuppressive therapy (e.g., corticosteroids, chemotherapy) may help improve immune function. However, this must be done carefully and under medical supervision to avoid rejection of transplanted organs or worsening of the underlying malignancy.
C. Management of Neutropenia
- If the patient has neutropenia (low neutrophil count), granulocyte colony-stimulating factors (G- CSF) may be considered to stimulate neutrophil recovery, especially in patients with hematologic malignancies undergoing chemotherapy.
4. Supportive Care
6. Prognosis
The prognosis of mucormycosis largely depends on several factors:
Drug Profile of Amphotericin B:
Mol wt-924.079g/mol Mol formula-C47H73NO17 B.P-804.34°C. M.P-170°C
Amphotericin B is one of the cornerstone treatments for mucormycosis, a severe and often rapidly progressive fungal infection caused by members of the Mucoraceae family. It is a broad-spectrum antifungal agent with potent activity against various fungal species, including Mucor, Rhizopus, and Absidia, which are the most common causes of mucormycosis.
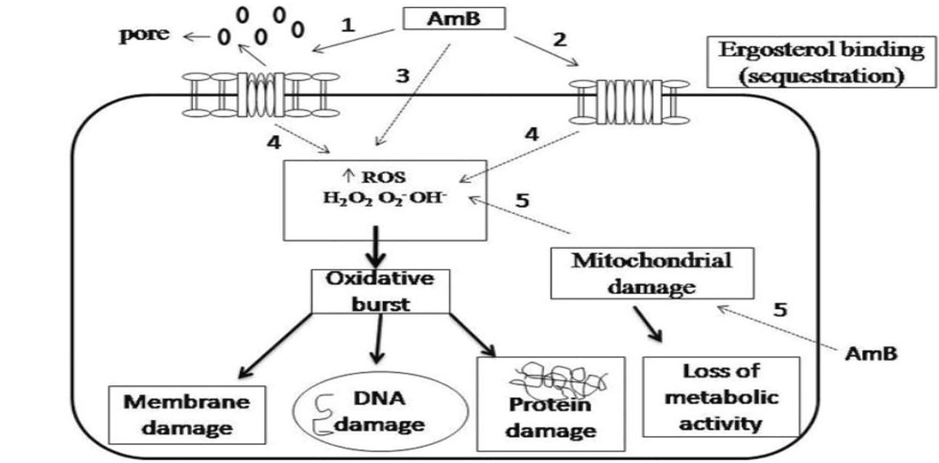
1. Mechanism of Action:
2. Pharmacokinetics:
3. Formulations of Amphotericin B:
There are several formulations of amphotericin B, and their selection depends on factors like side effect profile, severity of infection, and cost. These formulations include:
4. Indications for Use in Mucormycosis:
5. Dosing and Administration:
Conventional Amphotericin B:
Duration of Treatment:
CONCLUSION:
Mucormycosis is a serious, rapidly progressing fungal infection caused by the Mucorales family of fungi, which primarily affects immunocompromised individuals, including those with diabetes mellitus, hematologic malignancies, organ transplants, and severe trauma. The infection can lead to devastating complications, including tissue necrosis, vascular invasion, and dissemination to critical organs (e.g., brain, lungs, heart), often resulting in high morbidity and mortality if not diagnosed and treated promptly. The management of mucormycosis requires a multidisciplinary approach that combines aggressive antifungal therapy, surgical debridement, and careful management of underlying conditions. Early diagnosis is crucial and relies on a combination of clinical suspicion, microbiological testing, and imaging. Early intervention can improve survival rates significantly, but the disease's rapid progression means that diagnosis is often made in advanced stages, complicating treatment. Antifungal therapy with liposomal amphotericin B is the mainstay of treatment, though posaconazole and isavuconazole are emerging as alternatives, particularly for maintenance therapy or for patients unable to tolerate amphotericin B. The choice of antifungal and treatment duration is guided by the severity of the infection and the patient’s overall health. Surgical debridement of necrotic tissue is essential to control the spread of the infection and reduce fungal burden, especially for infections involving the sinuses, lungs, skin, and orbit. In some cases, more extensive procedures, such as amputation or orbital decompression, may be necessary to save life and preserve function.
REFERENCES






Sonkamble Sumed, Devshatwar Radhika*, Jamadar Amrata, Kamshette Arati, Akuch Sandhya, Survase Mohini, Clinical Review on Mucormycosis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 752-769 https://doi.org/10.5281/zenodo.15166601
 10.5281/zenodo.15166601
10.5281/zenodo.15166601