
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Malla Reddy College of Pharmacy, Dhulapally, Secundrabad, Telangana, 500100 (affiliated to Osmania University)
Introduction: Breast cancer is the most prevalent type of cancer to be diagnosed in women across the globe and also a significant issue with the major concern of public health in India where late diagnoses are prevalent. The lack of knowledge about risk factors and screening procedures contributes to delays in detection. The aim of the study was to measure the level of knowledge and awareness of the breast cancer in engineering students following a structured learning intervention. Methods: A quasi-experimental a pre-post intervention study was undertaken with undergraduate students of two Telangana colleges of engineering in India with the help of an educational intervention. The knowledge about the general awareness, symptoms, risk factors, and screening practices pre- and post-session were measured with self-administered questionnaire. Results: Out of the total number of participants (241) who took both tests, the baseline knowledge was improved after the intervention. The knowledge of breast cancer in men escalated significantly, 21.1% to 82.5%, and the awareness of the first symptom in the body escalated from 42.3% to 99.5%. The proper recognition of the key risk factors rose to 94.1% as compared to 90.4% and awareness of risk modifiable factors rose marginally by 51.0% as compared to 49.7%. Knowledge on screening also enhanced with correct answers on the frequency of BSE being at 65.9% compared to 56.8% and knowledge that early diagnosis can enhance survival rising to 62.2%. The overall post-intervention knowledge showed statistically significant better (p < 0.001). Conclusion: The organizational pharmacist facilitated educational intervention showed a significant boost in breast cancer knowledge amongst engineering students, highlighting the importance of awareness intervention that promotes early detection and healthy lifestyles.
Breast cancer is the most commonly diagnosed cancer among women in the world and it is a significant issue in the society. It is associated with a huge percent of cancer incidence and mortality as shown by world cancer statistics and it is a disease whose prevalence is on the rise in emerging countries like India [1]. As of 2020, breast cancer is the most frequently diagnosed cancer in the world, with 11.7 percent of all cancer cases. In 2022, cancer in the breast was diagnosed on approximately 2.3 million women and almost 670,000 deaths were documented across the globe [2]. Although there are increased survival rates in higher income countries, the disparities in the world are still major. In nations that have extremely high Human Development Index (HDI), 1 out of 12 women is likely to develop breast cancer in their lifetime and 1 out of 71 women succumb to breast cancer. Contrary to this, in low-HDI countries, 1 in 27 women are diagnosed but 1 in 48 women succumb to the disease which indicates poor survival rates because of late diagnosis and lack of access to treatment. Cancer remains a major cause of death in the world, despite the reduction in the mortality rate due to coronary heart disease and stroke [3].
Breast cancer in India is often diagnosed at advanced stages and thus it has a low clinical outcome and a high burden pertaining to treatment. The statistical data on the National Cancer Registry Programme (NCRP) of the Indian Council of Medical Research (ICMR) shows the high rural-urban disparity, with the incidence of cancer being about 5 per 100,000 in rural and 30 per 100,000 in urban regions. This is especially heavy in the metropolis cities and the northeast of the country. According to hospital-based cancer registry reports (2021) [4], gynecologic cancers, most of which is breast cancer, are almost half of all cancers in women. A number of reasons are associated with increased rates of breast cancer, namely, the evolution of lifestyle trends, late birth of a child, the lack of breastfeeding time, genetic precondition, and inaccessibility of structured screening systems. The pathogenesis of the disease is complicated and gradual, and it is difficult to prevent it on the primary level because of the participation of many cellular and molecular pathways. Thus, early diagnosis is one of the most useful measures that can be taken to decrease mortality and morbidity. The five-year survival rates differ greatly in India according to the stage of diagnosis; localized disease, 81.0% regional spread, 65.5% and distant metastasis, 18.3% [5]. Randomized controlled trials (RCTs), observational studies, analysis of failures and computational modeling have all shown the positive impact of mammographic screening on the outcome of breast cancer and mortality, and have thus provided the rationale to implement it in clinical practice. In addition, a meta-analysis of 11 trial randomized controlled trials found that mammography screening was linked to a potential decrement of about 20 percent in breast cancer specific deaths in women who were called upon to attend screening programs [9, 10].
Poor awareness about early warning signs, risk factors and screening modalities including breast self-examination (BSE), clinical breast examination (CBE) and mammography are some of the major factors that cause delayed diagnosis in India. False beliefs, social stigma, diagnosis phobia, and poor health literacy also deter the women to take action and obtain medical care promptly [2]. Risk factors that contribute to breast cancer include non-modifiable characteristics (biological sex, aging, hereditary susceptibility, genetic mutations) and modifiable characteristics (reproductive patterns (parity, age of first childbirth, breastfeeding habits) and lifestyle habits) [1,6]. These gaps are essential to bridge by means of awareness and educational interventions that would equip individuals with information on breast health and also promote proactive health-seeking behavior. Seminars conducted in institutions and communities have been proved to increase awareness, develop good attitudes towards screening and promote measures towards early detection. Higher institutions are particularly good locations to implement these kinds of projects given the fact that youths are the ones who visit the institutions and potentially increase the public health impact due to the potential transfer of the knowledge to their families and communities. [7].
Besides the creating awareness, responses of surveys that are conducted after educational interventions enable the participants to analyze their knowledge level on the baseline level, belief, and self-reported health status. Detecting self-reported breast-related complaints using such questionnaires can help detect those people who might need extra treatment or counseling. Moreover, the evaluation of the feedback responses will allow the researchers to determine the effectiveness of the awareness campaigns and find the areas of knowledge gaps that still persist and should be addressed with the help of targeted interventions. [8].
Consequently, the present study was aimed at measuring breast cancer awareness, self-reported symptoms, and opinions among college students who attended a lecture about breast cancer awareness. The research results of this work can be used to further comprehend the role of the educational program in creating awareness of breast cancer and promote the implementation of regular awareness and screening programs within academic institutions.
Study Aim
This research was aimed at measuring the level of breast cancer awareness, self-reported breast related symptoms and the attitude of early detection and health-seeking behavior in three participants in a breast cancer awareness lecture in one of the colleges.
Study Objectives
2. METHODS AND MATERIALS
Study Site
The study was conducted at two engineering colleges located in Telangana, India. Undergraduate engineering students from both institutions were included in the study. The awareness program was conducted within the college premises after obtaining necessary permissions from the respective authorities.
Study Design
A quasi-experimental pre–post interventional study design was employed to assess the effectiveness of a breast cancer awareness program. The intervention consisted of an educational seminar on breast cancer, which included information on basic understanding of breast cancer, risk factors and early warning signs, Importance of early detection, screening methods, including mammography, Demonstration of Breast Self-Examination (BSE) using standardized steps
A structured, self-administered questionnaire was administered before the seminar (pre-session) to assess baseline awareness and after the seminar (post-session) to evaluate changes in knowledge and understanding. Participants were also encouraged to actively practice the BSE technique during the demonstration session. Participation was voluntary, and confidentiality of responses was ensured.
Study Population and Sample Size
The study population comprised undergraduate engineering students enrolled at two selected engineering colleges in Telangana, India. Students present on the day of the breast cancer awareness seminar and willing to participate were included in the study.
All eligible students attending the awareness program were approached using a convenience sampling method. A total of 386 students completed the pre-session questionnaire, while 462 students completed the post-session questionnaire. The difference in sample size between pre- and post-intervention assessments was due to variations in attendance, availability, and willingness to participate at the time of data collection.
Inclusion And Exclusion Criteria
Inclusion Criteria: The study included women aged 18 years and above, undergraduate engineering students who were present for the breast cancer awareness event, willing to participate, and who gave informed consent met the inclusion criteria. Both the pre-test and post-test questionnaires were to be completed by participants, and they had to be able to comprehend the language used.
Exclusion criteria: Excluded from the study were women under 18, students who did not give informed consent, were hesitant to participate, left the program midway, or were absent during the breast cancer awareness session were all excluded. Participants with prior formal training, incomplete or partially completed questionnaires, or failure to finish the questionnaire were not allowed to participate in the study.
Ethical Considerations
The deans of both colleges granted permission to hold the sessions. All students who took part in the study did it voluntarily and their written consent was obtained. The study's objectives were clearly communicated to each participant, and they were made aware that their participation would be completely anonymous, with no personal information collected. The data collected was kept strictly confidential and used only for this study.
Study Tools
Three main study tools were used for the present study:
3. RESULTS
A. Patient’s demographics and past practices
After a thorough evaluation and the exclusion of incomplete questionnaires, 441 participants who completed pre- and post-session questionnaires were selected for analysis. Table.1 shows that 13.3% (n=32) students aged 18years. 29.7%(n=71) students aged 19years. 46%(n=110) students aged 20years and 9.2%(n=22) students aged 22years. Only 17% (n=41) has attended breast cancer awareness campaigns or initiative, while 83.4%(n=201) had not.
Table 1. participants age and past practices
|
Sr. No |
Variables |
% |
|
1. |
Age |
|
|
|
18 years |
13.3% |
|
|
19years |
29.7% |
|
|
20years |
46% |
|
|
21 years |
9.2% |
|
2. |
Have you ever attended breast cancer awareness programs |
|
|
|
Yes |
17% |
|
|
no |
83.4% |
B. Impact on knowledge against general perceptions towards breast cancer.
Baseline knowledge regarding breast cancer was suboptimal and showed improvement following the awareness intervention. As mentioned in Table2. The proportion of participants who correctly identified what breast cancer is increased marginally from 57.7%(n=139) in the pre-session assessment to 58%(n=140) in the post-session assessment. A substantial improvement was observed in awareness that breast cancer can also occur in men, with correct responses increasing from 21.1%(n=51) before the session to 82.5%(n=199) after the session, indicating a marked enhancement in knowledge following the intervention. A statistically significant improvement was observed in post-intervention knowledge scores compared to pre-intervention scores (p < 0.001).
Table 2: general perception
|
Sr. no |
Variable |
Pre-session |
Post-session |
P value |
||
|
correct |
wrong |
correct |
wrong |
|
||
|
1. |
What is breast cancer |
57.7% |
42.3% |
58% |
41.9% |
<0.97 |
|
2. |
Can men get breast cancer? |
21.1% |
78.8% |
82.5% |
17.4% |
<0.001 |
C. Impact on knowledge of Symptoms and Warning signs.
Knowledge of breast cancer symptoms and early warning signs improved significantly after the educational session. As shown in table 3, Correct identification of the earliest warning sign of breast cancer increased from 42.3%(n=139) during the pre-session assessment to 99.5%(n=240) post-session, accompanied by a corresponding reduction in incorrect responses. Awareness that most early-stage breast cancers are painless also improved, with correct responses increasing from 57.6%(n=139) pre-session to 58.9%(n=142) post-session, reflecting improved recognition of early disease characteristics. Figure1 provides a graphical elucidation of this section. Participants' overall understanding of breast cancer symptoms and early warning signs improved statistically significantly (p < 0.001).
Table 3: Symptoms awareness of breast cancer
|
Sr. No |
Variable
|
Pre-session |
Post-session |
P value |
||
|
correct |
wrong |
correct |
wrong |
|
||
|
1. |
What is the earliest warning sign? |
42.3% |
57.6% |
99.5% |
0.49% |
<0.001 |
|
2. |
Most early-stage breast cancers are painless. (T/F) |
57.6% |
42.3% |
58.9% |
39% |
0.12 |
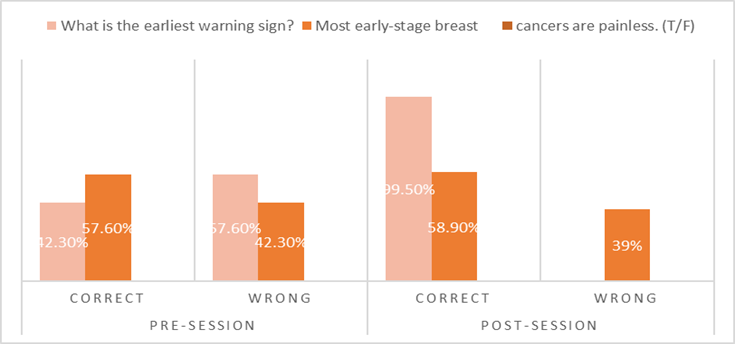
Fig1. Graphical representation of comparison between pre- and post-session knowledge regarding symptoms and warning signs.
D. Impact on knowledge of Risk factors
Participants’ understanding of breast cancer risk factors improved following the intervention. As shown in table 4, Correct identification of the major risk factor for breast cancer increased from 90.4% (n=218) in the pre-session assessment to 94.1% (n=227) post-session. Knowledge regarding the age group at higher risk of developing breast cancer showed a modest improvement, with correct responses increasing from 54.7% (132) to 55.1%.(n=44.8) Awareness of modifiable risk factors also improved slightly, with correct responses rising from 49.7% (n=120) before the session to 51% (n=123) after the session. Figure2 provides a graphical elucidation of this section. Participants' overall understanding of breast cancer risk factors improved statistically significantly (p< 0.003. p<0.002 and p<0.16).
Table 4: Risk factors awareness
|
Sr. No |
variable |
Pre-session |
Post-session |
P value |
||
|
correct |
wrong |
correct |
wrong |
|
||
|
1. |
What is the major risk factor for breast cancer |
90.4% |
9.5% |
94.1% |
5.8% |
0.003 |
|
2. |
What age group have higher risk of developing breast cancer |
54.7% |
45.2% |
55.1% |
44.8% |
0.16 |
|
3. |
What is the modifiable risk factor |
49.7% |
50.6% |
51% |
49.3% |
0.002 |
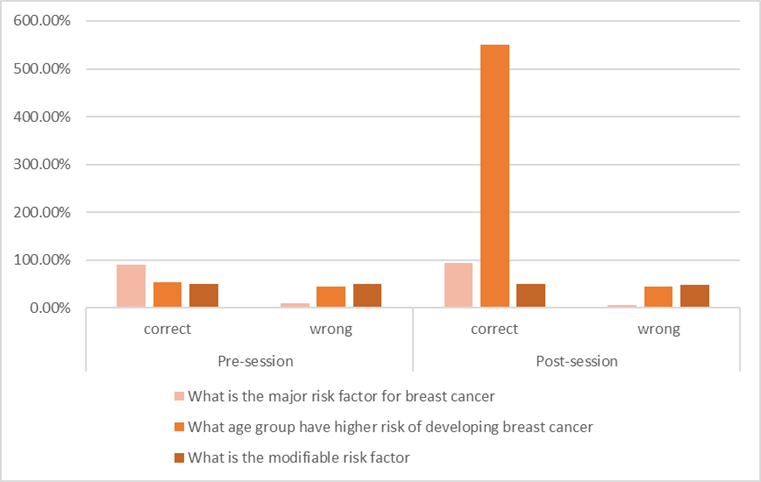
Fig 2. Graphical representation of comparison between pre- and post-session knowledge regarding the risk factors for breast cancer
E. Impact on Screening and Early detection
Awareness related to breast cancer screening and early detection increased notably following the awareness program. Correct responses regarding the recommended frequency of breast self-examination (BSE) increased from 56.8% (n=137) pre-session to 65.9% (n=159) post-session. Knowledge that early detection of breast cancer improves survival outcomes increased from 51% (n=123) before the intervention to 62.2% (n=150) after the intervention. Additionally, the correct understanding of the purpose of screening tests increased from 85%(n=205) pre-session to 86.7% (n=209) post-session, indicating improved comprehension of the role of screening in early diagnosis. Figure 3 provides a graphical elucidation of this section. Participants' overall understanding of breast cancer screening tests and early detection improved statistically significantly (p< 0.034. p<0.021 and p<0.16).
Table 5: Screening awareness on breast cancer
|
Sr. no |
variable |
Pre-session |
Post-session |
|
||
|
correct |
wrong |
correct |
wrong |
P value |
||
|
1. |
How often should women do BSE |
56.8% |
43.5% |
65.9% |
34.4% |
0.034 |
|
2. |
Can early detection of breast cancer increase survival rate |
51% |
49.3% |
62.2% |
38.1% |
0.021 |
|
3. |
What is the purpose of screening tests |
85% |
15.3% |
86.7% |
13.69% |
0.16 |
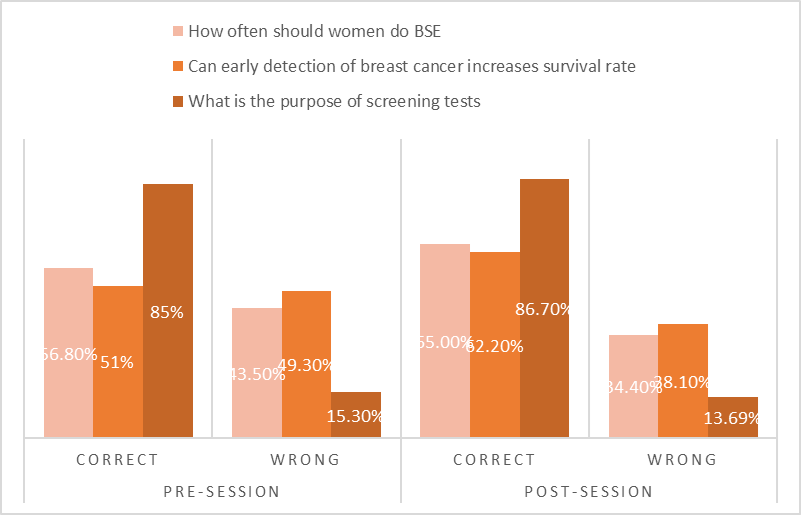
Fig3. Graphical representation of the comparison between pre- and post-session knowledge regarding screening and early detection.
DISCUSSION
The effect of the breast cancer awareness program on participants' overall knowledge scores was evaluated by comparing pre-assessment and post-assessment results using a paired samples t-test. The analysis included 241 participants who finished both tests, guaranteeing matched observations for precise within-subject comparison. After the educational intervention, descriptive statistics showed a definite increase in knowledge. With a median score of 4 and a mean pre-assessment knowledge score of 3.80 (SD = 2.48), the participants' baseline knowledge levels were comparatively low. The mean post-assessment score rose to 6.25 (SD = 2.78) with a median score of 6 after the awareness training, indicating a general improvement in participants' comprehension of ideas linked to breast cancer.
Table 6: Descriptive studies on overall awareness
|
Descriptives |
N |
Mean |
Median |
SD |
SE |
|
pre assessment |
241 |
3.80 |
4 |
2.48 |
0.159 |
|
Post assessment |
241 |
6.25 |
6 |
2.78 |
0.179 |
Paired sample T-Test
Table 7: Sample T-Test results
|
Assessment |
statistics |
Mean ± SD |
Mean Difference |
t (df) |
p-value |
Effect Size |
|
Pre vs Post |
-10.5 |
3.80 ± 2.48 vs 6.25 ± 2.78 |
−2.45 |
−10.5 (240) |
<0.001 |
0.675 |
The rise in knowledge scores seen following the intervention was statistically significant, according to inferential analysis. Pre- and post-assessment scores were significantly different, according to the paired samples t-test (t (240) = −10.5, p < 0.001). The two evaluations' mean difference was −2.45, with a standard error of the mean difference of 0.234, suggesting a trustworthy estimate of change. The statistical significance of the observed improvement was further confirmed by the mean difference's 95% confidence interval, which ranged from −2.91 to −1.99. Effect size analysis was used to assess the magnitude of the observed effect in addition to statistical significance.
A moderate to large effect size was suggested by the computed Cohen's d value of 0.675, indicating that the breast cancer awareness program significantly and meaningfully improved participants' knowledge scores. Overall, these results show that participants' knowledge of breast cancer improved significantly and in a clinically meaningful way after the awareness intervention, as seen by higher mean scores, narrower confidence intervals, and a strong effect size
Table 8: Complete case findings of pre-post interventional studies.
|
Domain |
PRE |
POST |
Difference |
P value |
||
|
Mean |
Standard deviation |
Mean |
Standard deviation |
|||
|
General awareness |
0.5 |
0.5 |
1.39 |
0.61 |
0.89 |
<0.001 |
|
Symptoms |
0.51 |
0.37 |
0.50 |
049 |
0.01 |
<0.017 |
|
Risk factors |
1.68 |
1.167 |
1.76 |
1.04 |
0.08 |
<0.04 |
|
Screening |
0.74 |
0.606 |
0.838 |
0.578 |
0.098 |
<0.07 |
Participants' knowledge about breast cancer improved statistically significantly across the majority of domains when compared before and after the intervention. Following the intervention, there was a very substantial increase in general awareness (p < 0.001), as well as significant improvements in knowledge about risk factors (p < 0.04) and symptoms (p < 0.017). Despite an increase in screening knowledge scores following the intervention, the difference was not statistically significant (p < 0.07). These results show that the awareness campaign was successful in raising awareness of breast cancer, especially in terms of risk factor recognition and general awareness.
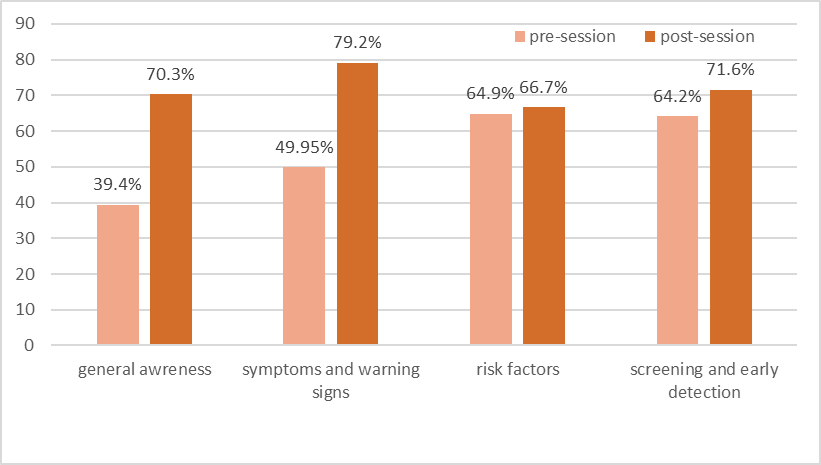
Figure 4. Graphical representation demonstrating the overall impact on knowledge
The graphical analysis shows that knowledge about breast cancer significantly improved after the awareness training in every domain that was assessed. Participants' general awareness of breast cancer significantly improved from 39.4% in the pre-session to 70.3% in the post-session.
Additionally, there was a significant increase in knowledge of symptoms and warning signs, from 49.5% prior to the intervention to 70.2% following the session, indicating better identification of early clinical features. From 64.9% in the pre-assessment to 66.7% in the post-assessment, participants' awareness of risk variables showed a slight increase, indicating a partial improvement that may have been brought about by their prior familiarity.
Additionally, screening and early detection knowledge grew from 64.2% to 71.6%, demonstrating a greater understanding of preventative measures and the significance of early diagnosis. The structured breast cancer awareness program was successful in raising participants' knowledge, as seen by the overall improvements seen in all domains. These results highlight the critical role that pharmacist-led educational initiatives play in raising community knowledge of breast cancer and encouraging early diagnosis and preventative health practices.
The study utilized a pre–post interventional design, enabling direct within-subject comparison and strengthening internal validity. Inclusion of participants from two engineering colleges enhances the external relevance of the findings within similar educational settings. The structured delivery of the educational intervention, including a standardized seminar and BSE demonstration, ensured consistency in content dissemination. Furthermore, the application of appropriate statistical analyses, including paired t-test and effect size estimation, adds methodological rigor to the study. The research also contributes valuable evidence by addressing breast cancer awareness in a non-medical student population.
CONCLUSION
The current interventional study shows that college participants' understanding of breast cancer was considerably increased by a structured program delivered by PharmD students. All assessed domains, including general knowledge of breast cancer, identification of symptoms and warning signs, knowledge of risk factors, and awareness of screening and early detection methods, showed a consistent increase in awareness when pre-assessment and post-assessment responses were compared. The post-session improvement that was noted demonstrates how well focused educational interventions can fill up knowledge gaps about breast cancer. The results highlight how important pharmacist-led community awareness campaigns are for encouraging early detection and preventive health behaviors. The program effectively improved participants' understanding of breast cancer-related concepts by providing evidence-based material through an interactive instructional approach.
The current interventional study demonstrates that a structured curriculum taught by PharmD students significantly improved college participants' comprehension of breast cancer. When comparing pre-assessment and post-assessment responses, there was a consistent increase in awareness across all assessed domains, including general knowledge of breast cancer, identification of symptoms and warning signs, knowledge of risk factors, and awareness of screening and early detection methods. The findings demonstrate the significance of community awareness initiatives conducted by pharmacists in promoting early detection and preventive health practices. The program successfully increased participants' comprehension of ideas linked to breast cancer by offering evidence-based content using an interactive teaching methodology.
ACKNOWLEDGMENTS
We are grateful to our institution's principal for allowing us to carry out the breast cancer awareness program and related research and for providing the institutional support we needed. The facilities and support offered were crucial to this study's successful conclusion. We sincerely thank the dean, the faculty of both engineering colleges for their approval, and all of the volunteers who helped make this study a success.
DATA AVAILABILITY STATEMENT: The original contributions made in the study have been included in the article/supplementary material.
Funding: No funding sources
CONFLICT OF INTEREST: None declared
REFERENCES

Shirley Angelina Kothur, K. V. S. Praneetha, G. Vyshnavi, K. Joyce Mary, Dr. M. Anusha, Impact of Clinical Pharmacist in Improving Breast Cancer Knowledge Through Educational Intervention Among Engineering Students: Evidence from Quasi Experimental Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 879-890. https://doi.org/10.5281/zenodo.18925360
 10.5281/zenodo.18925360
10.5281/zenodo.18925360