
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3 Assistant Professor, Department of Pharmacy Practice, Akshaya Institute of Pharmacy, Tumakuru
4,5,6 Final Year B Pharm, Department of Pharmacy Practice, Akshaya Institute of Pharmacy, Tumakuru
Type 2 diabetes is a major health issue in India. It occurs due to city life, obesity, lack of exercise, and genetics. Many people do not control their blood sugar well, leading to heart and kidney problems. Semaglutide (Ozempic), now available in India, helps manage blood sugar, weight, and heart health. It acts as a natural hormone, helping release insulin, lowering glucagon, slowing digestion, and reducing hunger. The drug lasts longer, requiring only weekly doses. Clinical trials from SUSTAIN showed significant reductions in HbA1c levels (up to approximately 1.8%), weight loss, and improved blood pressure and cholesterol levels. They also lowered heart and kidney risks in high-risk groups. Its safety profile matches other GLP-1 RA, with gastrointestinal issues being common side effects. Low blood sugar is rare unless insulin or sulfonylureas are used. Concerns exist about worsening eye problems and risks for those with thyroid cancer risk. In India, using semaglutide requires careful consideration of evidence and costs. It suits people with type 2 diabetes, obesity, heart disease, or kidney disease not responding to regular treatment. Careful dose adjustment, patient education, and monitoring ensure global evidence applies in India.
Diabetes Mellitus (DM) is a long-term metabolic disorder that arises when the pancreas fails to produce enough insulin or when the body is unable to use the insulin it generates effectively [1]. DM is a growing epidemic in the 21st century. More than 90% of diabetes cases globally are attributed to Type 2 Diabetes Mellitus (T2DM), and its occurrence is rapidly increasing in all areas, including India [2].
The International Diabetes Federation (IDF) Diabetes Atlas 2025 reports that around 629 million individuals globally are affected by diabetes, which significantly contributes to illness and death rates. This figure is expected to increase to 783 million by 2045, with low- and middle-income countries (LMICs) bearing the heaviest impact. Diabetes is categorised into type I, type II, and gestational diabetes mellitus, with T2DM being the most prevalent worldwide and the primary focus of this study. More than 90% of diabetes cases are T2DM, influenced by socio-economic, demographic, environmental, and genetic factors [1].Type 2 diabetes (T2DM) is marked by persistently high blood sugar levels, resulting from the pancreas's β-cells failing to produce and release enough insulin to satisfy the body's needs. Commonly, T2DM is linked to factors such as a family history of the condition, being overweight, leading a sedentary lifestyle, and being over the age of forty-five [3].Semaglutide, marketed under the brand names Ozempic, Rybelsus, and Wegovy, ranks among the most sought-after medications available. Produced by Novo Nordisk, semaglutide represents the latest addition to the class of glucagon-like peptide-1 receptor agonists (GLP-1 RA), primarily used for managing T2DM [4].The United States Food and Drug Administration (USFDA) approved Semaglutide (Ozempic) in 2017, followed by the European Medicines Agency (EMA) in 2018, to be used alongside diet and exercise for individuals with poorly managed T2DM [5].

Figure 1: Ozempic® (semaglutide) injection pen used for the treatment of T2DM.
Semaglutide is delivered via a prefilled pen as a subcutaneous injection once a week. It should be refrigerated until its initial use, but it can remain at room temperature for up to 56 days afterwards [6]. GLP-1, a key incretin hormone in humans, functions through various mechanisms, including enhancing insulin secretion in a glucose-dependent manner, inhibiting glucagon release, and reducing hepatic gluconeogenesis. Additionally, it slows gastric emptying and decreases appetite and energy consumption [7]. The identification of GLP-1 by Joel Habener and Svetlana Mojsov in the 1980s, along with Lotte Knudsen's development of long-acting versions of this hormone for obesity treatment in 2000, has been detailed by Friedman [3].
THE SCIENCE + POTENTIAL:
In 2017, the United States approved Ozempic for treating type 2 diabetes mellitus (T2DM). By 2021, Wegovy also received approval in the US as a medication for weight loss. As per Novo Nordisk, Ozempic is used alongside diet and exercise to enhance glycemic control in adults with T2DM. Both Ozempic and Wegovy are administered through a single-dose weekly injection, with doses of 0.5–2 mg and 2.4 mg, respectively. Semaglutide, the active ingredient, manages T2DM through multiple mechanisms. It aids in regulating blood sugar by imitating the GLP-1 hormone, which stimulates insulin production when blood sugar levels rise. Insulin facilitates the transfer of glucose from the bloodstream (extracellular) into the cells (intracellular), thereby reducing blood sugar levels. Additionally, semaglutide slows down gastric emptying and curbs appetite by affecting brain areas responsible for hunger and fullness signals [4].Semaglutide has been effective in managing T2DM and promoting weight loss. In the T2DM Sustain 7 Study, a clinical trial, patients who took Ozempic experienced a reduction in HbA1c—a measure of average blood sugar—by as much as 1.8% over 40 weeks [9]. An HbA1c level of 5.7% is considered normal; levels between 5.7% and 6.4% suggest prediabetes, and levels of 6.5% or above indicate diabetes. The HbA1c reduction observed in the Sustain 7 Study could potentially shift an individual from the diabetic range to a normal level of 5.7%. Beyond these advantages, research has also indicated a reduced risk of heart attack, stroke, and kidney failure in patients with T2DM [4].Over 90% of individuals with T2DM are either overweight or obese,1 and more than 20% of those with obesity also have T2DM. Certain medications prescribed for T2DM can cause weight gain, worsening this prevalent comorbidity. Weight loss plays a crucial role in managing T2DM, as it improves glycemic control and helps address related metabolic comorbidities [8].
Table 1. Commercial names, indications and administration of GLP-1 RAs [3]
|
Drug |
Brand Name |
FDA-Approved Indication |
Mode of Administration |
|
Exenatide |
Byetta |
T2DM |
SC, TD |
|
Bydureon |
T2DM |
SC, OW |
|
|
Liraglutide |
Victoza |
T2DM |
SC, OW |
|
Saxenda |
Obesity |
SC, OW |
|
|
Dulaglutide |
Trulicity |
T2DM |
SC, OW |
|
Lixisenatide |
Adlixin |
T2DM |
SC, OD |
|
Semaglutide |
Ozempic |
T2DM |
SC, OW |
|
Ribelsus |
T2DM |
Oral, OD |
|
|
Tirzepatide |
Mounjaro |
T2DM |
SC, OW |
|
Zepbound |
Obesity |
Abbreviations: OD=once daily; OW=once weekly; SC=Subcutaneous; TD=twice daily
Objectives and Scope of the Present Review:
Liraglutide was instrumental in the development of semaglutide, highlighting the potential of a modified long-acting GLP-1 analogue for treating diabetes and obesity. Building on liraglutide's achievements, semaglutide incorporates a fatty acid component to enhance albumin binding and reduce clearance. These structural refinements have increased albumin affinity, enabling once-weekly administration. In this discussion, we thoroughly explore the critical steps that led to the discovery and development of semaglutide, which was initially intended for T2DM and later recognised for its weight-loss advantages. To do this, we will draw on evidence from closely related fields such as medicinal chemistry and animal pharmacology [3].
Mode of Administration and Posology
Subcutaneous Route: In contrast to other weekly GLP-1 agonists, weekly subcutaneous semaglutide (Ozempic; 0.5 and 1.0 mg) requires dose titration. Treatment begins with a 0.25 mg dose, which is then increased to 0.5 mg and 1.0 mg, with each increment occurring every four weeks. The Ozempic pen comes in a concentration of 1.34 mg/ml and is available in red and blue versions. The red pen is used for the initial 0.25 mg dose and the 0.5 mg maintenance dose, while the blue pen is designated for the 1.0 mg maximum maintenance dose of semaglutide [7].
MECHANISM OF ACTION:[9]
Semaglutide is effective because it acts as a GLP-1 receptor agonist, imitating the function of natural GLP-1. This mechanism is crucial for comprehending both its advantages and the possible side effects associated with its use [9].
Glucagon-like-Peptide-1 Receptor activation:
Semaglutide interacts with and activates the GLP-1 receptor, a type of G protein-coupled receptor located on pancreatic β-cells, in the brain and within the gastrointestinal tract. This interaction initiates intracellular signalling pathways. It stimulates adenyl cyclase, which results in an increase in cyclic adenosine monophosphate, subsequently activating protein kinase A along with other signalling routes. Consequently, insulin secretion is elevated as a result. Therefore, semaglutide sets off a series of physiological reactions that are integral to its therapeutic benefits. This activation is fundamental to semaglutide’s mechanism, affecting various systems throughout the body [9].
Insulin secretion and glucose regulation:
When GLP-1 receptors are activated, semaglutide enhances insulin secretion from pancreatic beta cells, especially following food intake. This insulin release, which is dependent on glucose levels, is crucial for semaglutide's effectiveness in managing blood sugar without greatly increasing the risk of hypoglycaemia. At the same time, semaglutide reduces glucagon secretion from pancreatic alpha cells, a hormone that usually elevates blood sugar levels. This combined effect of insulin and glucagon helps achieve more stable and improved glucose regulation in individuals with T2DM [9].
Gastric emptying and appetite regulation:
Semaglutide delays gastric emptying, enhancing the sensation of fullness during meals and helping lower calorie intake. This effect, along with its impact on the brain's appetite centres, is vital to the drug's effectiveness in promoting weight loss. Beyond just slowing gastric emptying, semaglutide also affects the appetite centre in the hypothalamus by reducing the desire to eat high-calorie, appealing foods. This comprehensive approach to controlling appetite makes it an effective tool for managing weight [9].
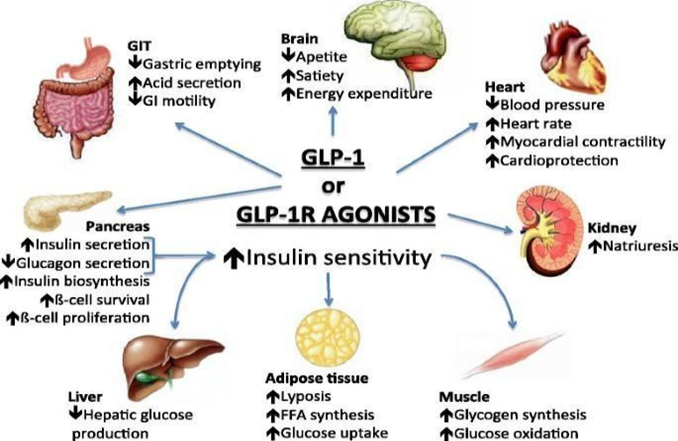
Figure 2: Effects of GLP1/GLP1-RAs on the different organs in the body [10]
Molecular Design and Rationale: [3]
The native incretin hormone GLP-1, a peptide composed of 30 amino acids, is swiftly released following meals and can enhance insulin secretion in a glucose-dependent manner. However, its pharmacological effectiveness is constrained by a plasma half-life of just a few minutes, mainly due to two factors:
DPP-4 enzymatically cleaves the Ala8–Glu9 bond in natural GLP-1. In semaglutide, the alanine at position 8 is replaced by 2-aminoisobutyric acid (Aib, also known as 2-methyl-alanine), an unnatural residue. This modification creates a steric hindrance that prevents DPP-4 from breaking down the analogue, thereby maintaining its biological function for several hours post-administration [3].Despite being resistant to DPP-4, short linear peptides are quickly cleared through glomerular filtration. To reduce this rapid renal clearance, a C18 diacid fatty chain was covalently linked to Lys26 using a spacer made of two 8-amino-3,6-dioxaoctanoic acid units and a glutamic acid component. This hydrophobic addition facilitates strong, non-covalent binding to circulating albumin, effectively transforming the plasma protein into a reversible storage depot and extending the terminal half-life to about one week. This duration is suitable for once-weekly (OW) dosing in humans, offering greater convenience compared to daily dosing schedules [3].A second substitution of Lysine with Arginine at position 34 removes a possible competing acylation site, ensuring that conjugation occurs solely at Lys26, thereby simplifying the purification process that follows. Besides these intentional alterations, the other residues were accurately aligned with GLP-1(7-37), maintaining the receptor-binding pharmacophore and retaining picomolar potency. The final free acid salt had an empirical formula of C187H291N45O59 and a molecular weight of 4113 Da, which is small enough for solid-phase peptide synthesis and large enough, post-acylation, to enable effective binding to serum albumin [3].
The three structural modifications—DPP-4 resistance, albumin tethering, and single-site acylation—offer several pharmacological benefits:
Thus, semaglutide is a peptide designed with precision, where its molecular alterations are directly aligned with the intended clinical outcomes: sustained blood sugar control, notable weight loss, and the convenience of once-weekly dosing without sacrificing safety or efficacy [3].
PHARMACOKINETICS OF SEMAGUTIDE: [5]
Absorption:
In healthy adults, a single subcutaneous dose of semaglutide 0.5 mg reaches its peak concentration (Cmax) within 24 to 56 hours. Studies involving dose escalation, where semaglutide was administered weekly at 0.25 mg for four weeks, then increased to 0.5 mg for another four weeks, and finally to 1.0 mg for five weeks, indicated a similar Cmax timing of 33 to 36 hours after the last 1.0 mg dose. The Cmax and the area under the plasma concentration–time curve (AUC) was comparable between a single 0.5 mg dose and the final 1.0 mg dose during the dose escalation process. Semaglutide's subcutaneous bioavailability is 94%, the highest among all currently available GLP-1 RAs [5].
Distribution:
Semaglutide was developed as a modified version of liraglutide, designed to have a stronger affinity for albumin, which enables it to be administered once a week. In a study by Lau et al. involving live pigs, it was found that the half-life of semaglutide after intravenous administration was about 46 hours, compared to 12 hours for liraglutide. Semaglutide exhibited a greater volume of distribution (0.102 L/kg versus 0.067 L/kg) and a slower rate of clearance (0.0016 versus 0.0038 L/h/kg), suggesting improved albumin binding. The average residence time after subcutaneous administration of semaglutide was around 63 hours, in contrast to 23 hours for liraglutide, yet the prolonged exposure to the drug did not result in any toxic effects [5].
Metabolism:
In a study examining the absorption, metabolism, and excretion of semaglutide, seven healthy male participants were administered a single subcutaneous dose of radiolabelled [3H]-semaglutide. The analysis of metabolites revealed that semaglutide was broken down into six distinct metabolites, identified as P1–P3 and P5–P7. The parent compound, [3H]-semaglutide, referred to as P4, was the predominant substance found in plasma, accounting for 82.6%. The metabolism of semaglutide involves proteolytic cleavage of the peptide backbone and beta-oxidation of the fatty acid side chains. Over time, the concentrations of metabolites decreased, with only the parent compound remaining detectable in plasma 28 days post-dosing. It remains unclear whether these metabolites contribute to the drug's effectiveness or its side effects [5].
Elimination:
In the same research, the elimination of radiolabelled [3H]-semaglutide and its breakdown products was documented. Following a single subcutaneous administration of 0.5 mg semaglutide, 75% of the dose was retrieved over a 64-day collection period. Of this, 53% was found in urine, 18.6% in faeces, and 3.2% in exhaled air. The original semaglutide compound and 21 metabolites were identified in the urine, with about 3% of the given dose being [3H]-semaglutide. Two metabolites, P6 and P7, each represented 14% of the administered dose, while all other metabolites accounted for less than 2% of the dose. The negligible presence of the intact drug in urine suggested that adjusting the dose based on renal function would not be necessary. No original drug was detected in the faeces [5].In a phase 2 clinical trial, hundred and fifteen subjects were randomized to subcutaneous semaglutide without dose escalation (0.1-0.8 mg QW) for 12 weeks or with dose escalation (0.4 mg steps to 0.8 or 1.6 mg over 1-2 weeks). The primary end-point was change in HbA1c from baseline; secondary end-points included change in body weight, safety, and tolerability.Semaglutide demonstrated a dose-dependent reduction in HbA1c from an initial level of 65 mmol/mol, decreasing it by up to 18.6 mmol/mol, and also led to a weight loss of up to 4.8 kg. More than 80% of participants achieved HbA1c levels below 53 mmol/mol. In an open-label study comparing liraglutide doses of 1.2 mg and 1.8 mg once daily, semaglutide at 1.6 mg showed superior reductions in HbA1c and weight, although it was associated with a higher frequency of adverse events (AEs) and withdrawals. The occurrence of nausea, vomiting, and withdrawals due to gastrointestinal AEs increased with higher doses of semaglutide, but most of these events were mild to moderate, temporary, and improved with dose escalation. There were no significant hypoglycaemic episodes, minimal injection-site reactions, and no unexpected safety or tolerability issues. Consequently, weekly doses of semaglutide at 0.5 and 1.0 mg with a 4-week dose escalation were chosen for phase 3 evaluations [5].
Clinical Progress:
T2DM: Application, Efficacy, and Side Effects
Clinical trial data on the use of Semaglutide in T2DM treatment: The Semaglutide Unabated Sustainability in Treatment of T2DM [SUSTAIN] clinical program comprises a series of Phase III trials designed to assess the effectiveness and safety of semaglutide across different patient groups. These trials included six major studies, primarily concentrating on the changes in HbA1c levels from the start to the conclusion of each trial, with durations ranging from 30 to 56 weeks. Participants included those who had not previously used medication, individuals on metformin or other oral antidiabetic drugs, and patients using insulin. Semaglutide was compared with placebo, DPP-4 inhibitors, other GLP-1RAs, and long-acting insulins. In each comparison, semaglutide consistently demonstrated significant reductions in HbA1c levels [11].Preclinical and pharmacokinetic studies in adults with type 2 established that semaglutide could be administered once a week. The drug's half-life was found to be around 7 days, ranging from 165 to 184 hours [12].
Evaluation of efficacy: Blood glucose control, improvement in insulin sensitivity, etc.
In several studies, administering semaglutide at a dose of 0.5 mg effectively lowered fasting plasma glucose (FPG) and postprandial glucose (PPG) levels. However, the 1.0 mg dose consistently achieved reductions in both FPG and PPG across all trials. Besides its glucose-lowering properties, semaglutide also enhanced beta cell function, as evidenced by increased fasting C-peptide levels and decreased glucagon levels. Improvements in insulin sensitivity were noted, with enhanced HOMA-B and reduced HOMA-IR observed in the SUSTAIN 1–3 trials [11].Moreover, semaglutide resulted in notable weight reduction, with losses ranging between 3.5 and 6.5 kg, contingent on the dosage and particular study. Additional advantages included decreases in systolic blood pressure (from 2.4 to 6.3 mmHg) and enhancements in lipid profiles in certain studies, although a minor rise in pulse rate was observed. Common adverse effects encompass gastrointestinal issues and hypoglycaemia [11].In the semaglutide clinical program, more than 8,400 individuals with T2DM were assessed across eight studies. The discontinuation rate due to adverse events (AEs) was generally low, ranging from 5% to 13%, except in the SUSTAIN 6 trial, where it rose to 20%, likely because of its extended duration. The primary reasons for discontinuation were gastrointestinal AEs, including nausea, diarrhoea, and vomiting. Hypoglycaemia was uncommon, except when semaglutide was combined with insulin or sulfonylurea. There was no notable increase in calcitonin levels or cancer risk. Although semaglutide has been effective in reducing diabetic nephropathy, it is linked to a higher occurrence of diabetic retinopathy, probably due to the rapid decrease in HbA1c [11].Long-term safety evaluations and cardiovascular risk analysis were conducted. In a randomised study with 3,297 T2DM patients, the impact of the GLP-1 medication semaglutide was compared to a placebo over a period of 104 weeks to assess cardiovascular outcomes. The findings indicated that the primary composite endpoint, which included cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke, was lower in the semaglutide group compared to the placebo group, establishing its noninferiority. Additionally, while semaglutide was effective in lowering the risk of kidney disease, it was linked to a higher occurrence of diabetic retinopathy complications. Overall, semaglutide demonstrated an acceptable safety profile and offered cardiovascular protection. These findings endorse its role as a significant treatment option for patients with T2DM, while highlighting the importance of monitoring for retinal complications to ensure its safety [11].
Safety Profile and Tolerability:
Similar to other GLP-1 receptor agonists, semaglutide is not recommended as an initial treatment due to the potential risk of thyroid cancer, as indicated by animal studies.1 It should be avoided in individuals with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia, T2DM. While semaglutide is generally well tolerated, with dropout rates comparable to placebo, it may be less tolerated than dulaglutide (Trulicity). The most frequent side effects include nausea, vomiting, and diarrhoea, affecting about 30% of patients, typically when the dosage is increased. Around 3% to 4% of patients may stop treatment due to gastrointestinal side effects [6].Individuals who take Ozempic for weight loss may be at an increased risk of various health problems, including gastrointestinal problems [13].
Table 2: Serious side effects and Adverse Drug Reactions (ADRs) [10]
|
Serious side effects |
ADRs |
|
gastrointestinal contraction) |
Management of side effects:
Thyroid cancer boxed warning: At present, the likelihood of getting thyroid cancer is low. Nonetheless, if you experience symptoms like neck lumps or swelling, hoarseness, breathing difficulties, or trouble swallowing, it is crucial to seek medical attention promptly, as these could be signs of thyroid cancer [10].Recent data indicate that semaglutide injections, marketed as Ozempic and Wegovy, are increasingly being prescribed for weight management and diabetes, as well as for regulating blood sugar levels in individuals with T2DM. However, recent research has highlighted concerns regarding its side effects, particularly the potential for thyroid tumours, including medullary thyroid carcinoma (MTC). An important FDA warning pointed out that laboratory animals given semaglutide developed thyroid tumours, though the risk to humans is still uncertain [13].
Abdominal pain and gallbladder disease: When semaglutide is prescribed, it is crucial to monitor symptoms such as persistent abdominal pain that extends to the back and is accompanied by vomiting, as these may necessitate urgent medical intervention. Additionally, patients should be observed for signs such as fever, jaundice, or clay-coloured stools, as these could suggest gallbladder issues and require immediate attention [10].
Visual changes: During semaglutide treatment, monitor patients for visual changes. An annual comprehensive eye examination with dilation is advised [10].
Hypoglycaemia: Semaglutide should be used cautiously when combined with other glucose-lowering drugs, such as sulfonylureas (e.g., glibenclamide) or insulin, due to the potential for increased hypoglycaemia risk. Indicators of hypoglycaemia can include severe hunger, trembling, confusion, dizziness, blurred vision, a rapid heartbeat, and mood swings. Consistent monitoring of blood sugar levels can help manage the risk of hypoglycaemia [10].
Kidney impairment: Excessive fluid loss due to diarrhoea, nausea, and vomiting can result in dehydration, potentially exacerbating kidney damage or existing kidney issues. It is important for patients to be advised to consume ample fluids to mitigate the risk of dehydration [10].It is established that between 23% and 43% of individuals with T2DM go on to develop CKD, and at present, diabetes is the leading cause of end-stage kidney disease (ESKD) necessitating renal replacement therapy. Furthermore, albuminuria is detected early in the diagnosis of T2DM in 17% to 26% of patients. Those with T2D and CKD who experience macroalbuminuria face a higher risk of dying from cardiovascular disease compared to those who advance to ESKD [14].
Hypersensitivity: Individuals may experience severe hypersensitivity or allergic reactions, which can manifest as skin rashes, itching, swelling of the face (including lips, tongue, or throat), difficulty breathing or swallowing, fainting, or feeling lightheaded with a rapid heartbeat. These side effects might continue even after stopping semaglutide, particularly when it is administered at the highest dose of 2 mg [10].
Contraindications: [10]
Warning and Precautions: [10]
Indian Regulatory Status, Pricing and Access:[15]
In December 2025, Ozempic (subcutaneous semaglutide) was introduced in India, available in prefilled pens that administer doses of 0.25 mg, 0.5 mg, and 1 mg on a weekly basis. The initial 0.25 mg dose is priced at ?2,200 per week (?8,800 monthly), while the 0.5 mg and 1.0 mg doses are priced at ?10,170 and ?11,175 per month, respectively. It is approved for use as a supplement to diet and exercise for adults with poorly controlled T2DM, with the added benefit of promoting significant weight loss and reducing cardiorenal risks in high-risk patients.
Translating Global Evidence into Indian Practice:
Future directions and research needs in India:
This review investigates the broadening applications and therapeutic challenges of GLP-1 receptor agonists, with a particular emphasis on their influence on muscle mass and chronic illnesses. It explores the dual nature of the benefits and obstacles presented by GLP-1 therapies, offering insights into the associated therapeutic strategies and potential future research paths. This topic is highly relevant due to the escalating global incidence of obesity and related metabolic disorders. The emergence of a new domain for GLP-1 receptor agonists (GLP-1RAs) highlights the widening scope of these drugs, which now includes single, dual, and triple agonists that target GLP-1, GIP, and glucagon receptors, aiming to achieve enhanced therapeutic outcomes beyond mere glucose regulation and weight reduction [16].
GLP-1RAs play a role in metabolic imbalances by enhancing insulin release, slowing gastric emptying, and reducing appetite. Ongoing and dedicated research is uncovering their therapeutic advantages for conditions like obesity, cardiovascular disease, chronic kidney disease, and non-alcoholic steatohepatitis (MASH), as well as their effects on neurodegenerative disorders and substance use issues. This article offers a thorough spatiotemporal analysis and evaluation of the dual nature of GLP-1 treatments, highlighting both their potential benefits and risks. Balancing these aspects is crucial due to the widespread use of these medications across various medical fields. This balance can be effectively addressed within current academic discussions by examining the gaps in existing knowledge and conducting a comprehensive systematic review of research outcomes [16]. In conclusion, this study makes a valuable contribution by examining the evolving field of GLP-1 therapies and highlighting the need to balance therapeutic benefits with associated risks and consequences, particularly in preserving muscle mass. It serves as an important reference for clinicians, pharmaceutical companies, and researchers to understand current and future trends in the management of chronic disorders using GLP-1 therapies [16].Ongoing research on tirzepatide is focused on its application for cardiovascular diseases and metabolic-associated steatosis liver disease (MASLD), building on its approved use for type 2 diabetes and obesity. Studies are delving into its mechanisms, efficacy, and potential benefits, particularly as a less invasive alternative to surgery for these conditions, showing promising results in reducing liver fat, enhancing metabolic indicators, and lowering the risk of liver and heart complications. This review highlights a significant concern about the possible negative impact on muscle mass, offering valuable insights into the debates within the medical and pharmaceutical communities [16].Additionally, emphasizing the need to establish protective measures for protein consumption and resistance training underscores comprehensive strategic patient care, whether in formal or strategically ambiguous contexts. It also points to future pathways, advocating for proactive initiatives to enhance resilience in current research and innovation [16].
Ideal Candidates in India:
Given the robust global evidence and the limitations of cost and availability, Indian doctors will need to prioritise semaglutide for patients most likely to gain wide-ranging benefits. Ideal candidates include
In many cases, semaglutide may be considered for patients after metformin, an SGLT2 inhibitor, and one or more other oral medications have not been effective, potentially taking the place of sulfonylureas to minimise hypoglycaemia and weight gain, or as an alternative to further increasing insulin therapy. For certain high-risk individuals, the early introduction of GLP-1 RA in combination with metformin and SGLT2 inhibitors could be warranted, though this decision will rely on personal financial capacity and collaborative decision-making [17].
Practical Initiation and Monitoring:
In Indian medical practice, Ozempic is typically initiated at a dose of 0.25 mg weekly once for the first four weeks. After this period, the dosage is increased to 0.5 mg, with the possibility of further raising it to 1.0 mg if the desired glycemic and weight goals are not achieved and the patient tolerates the medication well. Healthcare providers should assess the doses of any concurrent sulfonylurea or insulin to minimise the risk of hypoglycaemia, offer guidance on diet and lifestyle changes, and instruct patients on injection methods and potential gastrointestinal side effects [18].During follow-up appointments, it is important to track HbA1c levels, fasting and post-meal glucose, body weight, and blood pressure, as well as watch for any signs of pancreatitis or gallbladder issues. Patients should be encouraged to stick with the treatment despite initial side effects like temporary nausea or decreased appetite. For many Indian patients, the cost will significantly influence their ability to continue treatment, so healthcare providers might need to discuss realistic therapy durations, possible step-down plans, and alternative options if long-term affordability is a concern [18].
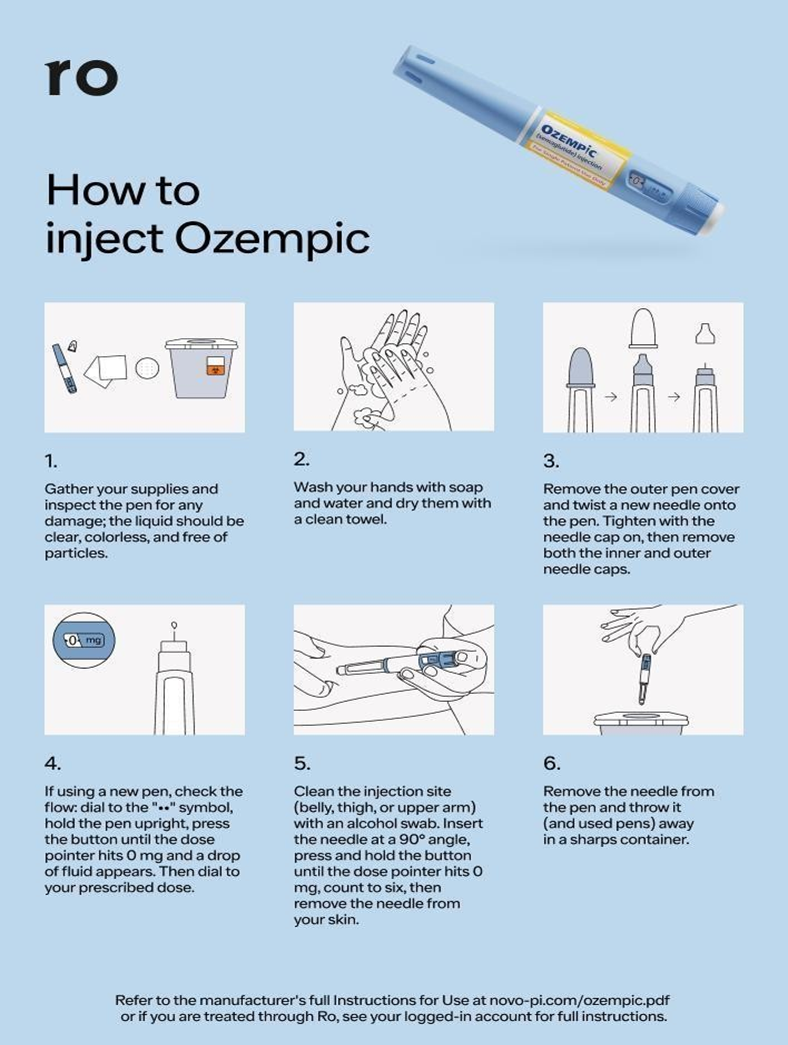
How to Inject Ozempic:[19]
CONCLUSION:
This review shares key information about the prevalence of type 2 diabetes (T2DM). Semaglutide is a drug used to treat diabetes. It works by activating the GLP-1 receptors. This review discusses the discovery of semaglutide, its development, clinical studies, role in treatment, practical use, recent updates, and its efficacy. Clinical trials have shown that semaglutide is effective and safe in adults, older people, and obese patients with type 2 diabetes. This includes patients with kidney, liver, or heart problems. Although semaglutide often causes stomach issues, it is generally well-tolerated. Semaglutide represents a significant advancement in the treatment of T2DM and obesity. It helps control blood sugar, aids weight loss, and reduces heart risks.Rare but serious side effects, like pancreatitis and thyroid tumours, require careful monitoring and choosing the right patients. The long-term safety of semaglutide is still being studied. Although current data look good, more research and monitoring after the drug is on the market are needed to fully understand its long-term effects and improve its use for different patients.
REFERENCES:





Dr. Shivaraj D. R.1*, Dr. Nagarjuna D.2, Dr. R. S. Meghasri3, Varshini J.4, Gowthami L.5, Bharath Gowda H. G.6, Injectable Semaglutide (Ozempic) For Type 2 Diabetes in India; Traslating Global Evidence into Real-World Practice After Recent Market Entry, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 592-605. https://doi.org/10.5281/zenodo.18485151
 10.5281/zenodo.18485151
10.5281/zenodo.18485151