
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Rungta Institute of Pharmaceutical Sciences
Cognitive impairment, often known as cognitive decline, can occur gradually or suddenly, and it may be temporary or more permanent. It is a growing public health problem and may rely on normal age or be linked to other neurological conditions like Alzheimer's disease (AD). It is now commonly acknowledged that lifestyle variables, including eating habits, have a significant role in supporting good aging and minimizing cognitive impairment in later life. Among the natural substances that have gained a lot of interest recently are dietary polyphenols, which comprise phenolic acids. Improved cognitive function and the avoidance of cognitive deterioration have been associated with their supplementation. Despite their therapeutic potential, there is a dearth of human studies investigating the connection between phenolic acid ingestion and cognitive outcomes. In this review, we provide preclinical evidence that a variety of dietary polyphenols, such as ellagic acid, rosmarinic acid, and cinnamic aldehyde, can have pro-cognitive and neuroprotective effects through a variety of molecular mechanisms, including the control of inflammatory status and pro-oxidant and antioxidant machinery. To support the promising preclinical results, more thorough in vivo study is needed. Although phenolic acids have good pharmacokinetic qualities and can accumulate in the brain at pharmacologically relevant levels, future research should identify which of the different metabolites produced because of phenolic acid consumption may oversee the potential neuroprotective effects of this subgroup of polyphenols.
Nootropics, often known as smart medications, are well-known substances or supplements that improve cognitive function. They function by improving mental abilities like motivation, creativity, memory, and concentration.[1] They function by improving mental abilities like motivation, creativity, memory, and focus. The goal of recent studies was to identify a novel possible nootropic made from both natural and manmade materials. Numerous studies have been conducted on the impact of nootropics on the brain. The dopaminergic pathway is one of the processes or paths via which the nootropic influences brain function. Nootropics have been shown to have an impact on the treatment of memory disorders, including Parkinson's, Alzheimer's, and Huntington's illnesses. It has been noted that those illnesses affect the same nootropic pathways. There are two types of nootropics: natural and herbal nootropics like Panax quinquefolia’s (American ginseng) and Ginkgo biloba, and synthetic nootropics like piracetam. It has been demonstrated that using natural nootropics can improve brain health and function. Nootropics work against the brain's tiny arteries and veins by acting as vasodilators.[2] Incorporating natural nootropics into the system will improve blood flow to the brain while also supplying vital nutrients, energy, and oxygen.[3] The brain receives about 15% of the body's total blood flow and oxygen, although making up only 3% of the body weight. In actuality, the brain can only produce energy by burning glucose, demonstrating that neurons require a steady flow of nutrients and oxygen.[4] Unlike most other bodily cells, neurons are unique and cannot be replicated. The converted energy is continuously being used by the neuron cells to keep the cell compartments repaired. The energy produced by the glucose is essential for neurotransmitter, electrical, and maintenance functions.[5] It has also been demonstrated that natural nootropics could lessen brain inflammation. Nootropics will minimize the consequences of brain aging and shield the brain from poisons. The activation of new neuron cells is another way that natural nootropics improve brain function. The brain becomes more active because of the new neural cell's motivation, which improves thinking and memory skills and increases neuroplasticity.[6] Acetylcholine is the primary neurotransmitter in the peripheral, autonomic, and enteric nervous systems and was the first neurotransmitter discovered in the history of neuroscience.[7] The "cholinergic hypothesis of cognitive dysfunction" was developed as a result of preclinical and clinical evidence, as well as the observation of a decrease in choline acetyltransferase, an enzyme involved in the biosynthesis of acetylcholine, in the cerebral cortex of Alzheimer's disease patients. Different classes of medications, including acetylcholinesterase/cholinesterase inhibitors, cholinergic antagonists of muscarinic receptors, muscarinic cholinergic inhibitors, and acetylcholine precursors, were developed based on this hypothesis and the relationship between brain levels of acetylcholine and cognitive performance.
Cognitive Impairment or Neuro-degradation:
Cognitive impairment is a symptom or description of thinking problems (memory, focus, judgment), whereas neuro-degradation refers to the underlying physical breakdown of brain cells or tissue, which is often the cause of severe cognitive decline (neurocognitive diseases, dementia, Alzheimer's). Mild impairment (MCI) is less severe than significant neurocognitive illnesses, but it might increase the risk of dementia. In essence, cognitive impairment (difficult thinking) is produced by neuro-degradation (such as neuron loss). Neurodegenerative illnesses, such as Parkinson's disease, Alzheimer's disease, Lewy-body dementia, and cerebrovascular dementia, cause a gradual decline in behavior and cognition that ultimately results in severe dementia. By 2050, there will be 1.1 billion persons over 65 worldwide, according to current demographic projections, which will result in 37 million cases of dementia. Given the enormous public health and socioeconomic burden, it is evident that the need of therapeutic intervention aimed at either finding a cure or preventing sickness onset cannot be stressed. Nowadays, the human population is aging faster. This leads to increased dependence rates, and social and health services need to adapt to this aging population. One of the changes this group has experienced is frailty. It is characterized as a syndrome that is clinically detectable and linked to the aging of many physiological systems that result in a state of vulnerability. The pathophysiology of frailty, which seems to have a complicated genesis, is determined by a number of interrelated elements. The four main causes of frailty, according to Morley et al., are atherosclerosis, sarcopenia, cognitive decline, and malnutrition, together with the associated metabolic alterations. Malnutrition is associated with cognitive impairment or functional loss, while inadequate nutrition is known to predispose to cognitive fragility. Additionally, dietary factors that may impact vascular risk factors may worsen dementia in people with cognitive fragility. This study aims to provide an overview of the nutritional components that have been investigated thus far and that may be involved in the development of frailty, namely cognitive impairment. The progressive dysfunction of specific neuronal groups determines the clinical manifestation of neurodegenerative illnesses. Misfolded proteins accumulate both intracellularly and extracellularly in many neurodegenerative protein-pathies, which is associated with neuronal death. Some of the main fundamental processes include deficiencies in the ubiquitin-proteosome-autophagy system, oxidative stress and free radical production,mitochondrial dysfunction, impaired bioenergetics, neurotrophin dysfunction, "neuroinflammatory" processes, and (secondary) disruptions of neuronal Golgi apparatus and axonal transport. Over an extended period of time, a number of interrelated events culminate in programmed cell death. Current study has shown both intraindividual variances and overlap across diverse symptoms, despite the fact that neurodegenerative disorders are classified using major components of protein deposits or established genetic mechanisms. Synergistic mechanisms between sick proteins reveal common pathogenic pathways. The basic mechanisms of neurodegeneration and cell death have been clarified by animal models and other research, creating new opportunities for preventative and therapeutic strategies.
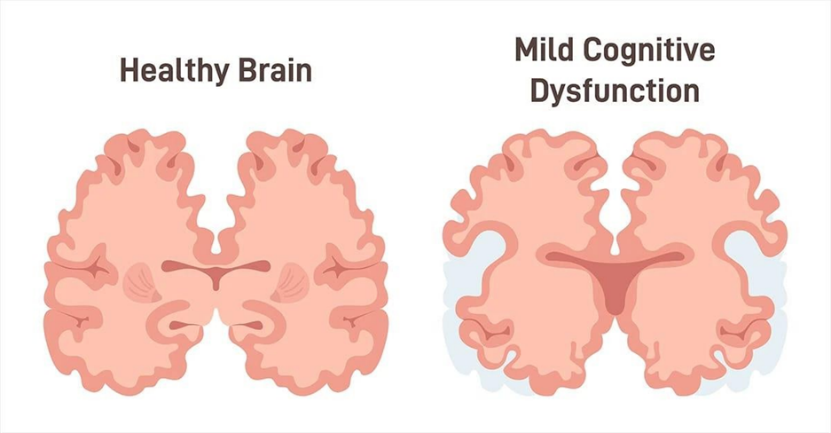
Fig: 1.1Difference between Normal Brain and Damaged Brain
The greatest consistent risk factor for developing a neurodegenerative disease, especially AD or PD, is becoming older. Over the past century, the number of people in developed countries who are 65 years of age or older has increased far more quickly than the total population. Consequently, it is anticipated that over the next few generations, the number of elderly people would double, which could lead to an increase in the number of persons suffering from neurodegenerative disorders.Management of Alzheimer’s disease
The Frailty Concept:
The world's population is quickly aging, which leads to the development of illnesses connected to aging. Neurological disorders were the primary cause of DALYs (disability-adjusted life-years), the second most prevalent cause of mortality (90 million), and the sum of years of life lost (YLLs) and years lived with disability (YLDs) (276 million), according to recent reports.
One of them that geriatric medicine has recently concentrated on is frailty. A person's heightened vulnerability to stressors resulting from deterioration in several physiological systems is a clinical condition known as frailty. Frailty is a physical, social, and cognitive illness that is a condition of reversible pre-disability. A standard definition of frailty was sought by Fried et al.
Described the situation of being more vulnerable to homeostatic resolution after a stressful experience as a clinical characteristic of frailty. For senior individuals living in the community, this increases the likelihood of unfavourable outcomes, such as falls, disability, fractures, hospitalization, and death. A secondary analysis of data from 5210 men and women over 65 who took part in a prospective cohort study known as the Cardiovascular Health report served as the basis for the initial report.
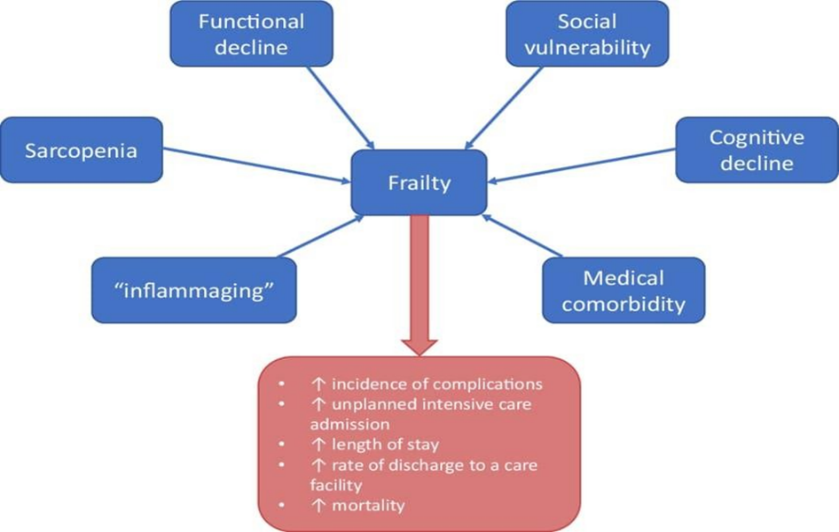
This concept has been widely used and mostly focuses on the physical features. A set of five criteria (weight loss, weariness, sedentary behaviour, sluggish walking, and low physical strength) are used to thoroughly assess the presence or absence of signs or symptoms. Pre-physical fragility is characterized by one or two of these traits, while physical frailty is characterized by three or more of these five prerequisites. Numerous factors impact the pathophysiology of frailty, and its genesis seems to be complex. The four main causes of frailty, according to Morley, are atherosclerosis, cognitive decline, malnutrition, and sarcopenia with associated metabolic issues.
Dementia is another common health problem among the elderly. Moreover, cognitive impairment is considered a component of frailty. Physical frailty and dementia or cognitive impairment have been demonstrated to be strongly correlated in a number of cross-sectional and longitudinal investigations.
Sign and Symptoms:
Language and problem-solving difficulties, memory loss, emotional or behavioral problems, and difficulty focusing are signs and symptoms of cognitive impairment. These problems can make everyday tasks more challenging and are more serious than typical age-related forgetfulness. Repeating the same stories or having difficulty following a recipe or handling money are examples of specific symptoms.
1. Learning, focus, and memory.
2. Language and Communication.
3. Making choices and using judgment.
4. Shifts in mood and behaviour.
5. Disorientation and confusion.
6. A visual issue.
Causes:
Aging, illnesses, lifestyle choices, and injuries are some of the factors that contribute to cognitive impairment. Age-related changes are the primary cause, but other contributing factors include diseases including Alzheimer's, Parkinson's, and stroke, infections, vitamin deficiencies, depression, long-term alcohol or drug misuse, and head injuries. To identify the specific cause of the right course of treatment, a proper diagnosis is essential.
• Health issues:
Mechanism:
Neurotransmitters are not released by nootropics, nor do they function as receptor ligands. [8]
but enhance the brain's oxygen and glucose flow, have ant hypoxic properties, and shield brain cells from neurotoxicity. [9,10] Additionally, they improve the production of proteins and nucleic acids in neurons and promote the metabolism of phospholipids in neurohormonal membranes. [11,12] Certain nootropics have been shown to enhance erythrocyte flexibility, have an anti-aggregation impact, and influence the removal of oxygen free radicals. This enhances blood flow to the brain and improves the blood's rheological characteristics. [13,14,15] Although these drugs are metabolically active, most nootropics don't work right away after a single dose and need to be used for a long time to demonstrate any effects. To enhance brain metabolism, they must be able to cross the blood–brain barrier, and sustained use is required to have long-lasting effects. [16] example of piracetam as a nootropic effect-
Important neurotransmitter modes of action include:
The manipulation of neurotransmitter systems such acetylcholine, dopamine, serotonin, glutamate, and GABA is one of the main ways that nootropics improve cognition. They accomplish this via influencing cellular metabolism, receptor sensitivity, and neurotransmitter availability, among other mechanisms.
Types Of Nootropic Drugs:
Nootropic medicines, also known as "smart drugs," are a broad family of drugs that can improve brain function and are typically grouped according to their source and purpose. They fall into three general categories: synthetic over-the-counter agents, natural chemicals, and prescription drugs.
1. Supplemental (Natural Nootropics): These substances come from organic sources including plants, herbs, and nutrition. Compared to prescription medications, they are freely accessible over the counter and typically have less potency but fewer negative effects.
Herbal Remedies:
2. (OTC) investigational synthetic nootropics: These are substances made in laboratories, many of which don't need a prescription but aren't usually FDA-approved for use as cognitive enhancers in healthy people.
A. racetams: class of synthetic substances known as racetams, of which piracetam was the first nootropic to be produced. They function by influencing the glutamate and acetylcholine neurotransmitter systems. Examples consist of:
Piracetam Aniracetam
Pramiracetam
Oxiracetam Additional Synthetics
B. Noopept: Often marketed as a supplement, this peptide affects glutamatergic signaling, albeit it isn't accessible in the US.
B. Citicoline: A substance that helps with learning and memory, especially in elderly adults recovering from stroke or experiencing mild cognitive impairment.
3. (Pharmaceutical Prescription) Nootropics: These powerful, synthetic drugs are used to treat certain illnesses like dementia, narcolepsy, and ADHD. Although they are more likely to cause adverse effects and dependence, they often have bigger effects.
Indications:
Nootropics are used to treat memory, consciousness, and learning impairments in acute or subacute circumstances.[17] They are advised for early brain injury, which shows up as mental retardation, memory loss, and qualitative alterations in consciousness. Acute psychoorganic syndrome (POS) is the term used to describe this disease. Although it is typically curable, in certain instances it may develop into dementia. Brain injury, infection, stroke, or intoxication (alcohol, medications with central anticholinergic action, or carbon monoxide) can all result in acute POS. The POS category also includes delirium tremens.[18] Chronic cognitive issues including mental retardation or memory impairment could be further signs. In these situations, nootropics are used somewhat often, but their usefulness is debatable, particularly in cases of more severe dementia. When there is merely a slowing down of brain function without the development of dementia, such as in people with minor cognitive impairments or "benign senescent forgetting," they appear to be more beneficial. [19,20] Fatigue and exhaustion-related attention and memory problems can occasionally be treated using nootropics.[21,22] Children with mild brain dysfunction syndrome also utilize them.[23,24]
Nootropic Treatments:
In general, nootropics are quite well tolerated. The dosage determines their effectiveness, and in reality, giving too little of a dose is a frequent error. After the disruption of consciousness has subsided, treatment should continue for a minimum of two to three weeks [25]. To measure the extent and duration of impaired consciousness, a clinical scale has been created. Eye-opening, verbal performance, and motor responsiveness are three behavioral elements that are tested separately. These are noted and regularly assessed in accordance with the chart [26]. Nootropic side effects are rare and seldom dangerous. In addition to individual intolerance, there may occasionally be an increase in libido, a sleep disturbance, or an increase in activity in the undesired direction.
Advantages and Disadvantages of Natural Vs Synthetic Nootropics:
Natural origin medications derived from various plant parts (flower, leaf, root, etc.) have the undeniable advantage of having a wider range of potentially advantageous pharmacological effects. This is because a herbal medication contains a variety of compounds that can have additive or synergistic effects.[27] Additionally, natural nootropics are typically less toxic, which lowers the risk of overdose injury. Certain substances, however, could lessen the pharmacological activity of other substances.[28] Plant extracts are frequently utilized since higher doses of such a herbal medication are required to provide the intended effect. Additionally, there are issues with storage, potential falsification, and authenticity verification. [29,30] The pharmaceutical purity, specificity of action, and potential for increased effect through chemical structural alteration are the benefits of synthetic substances.[31] Although they are typically active at lower dosages, there is a higher chance of overdosing.[32]
Herbal Drug Plant Collection for the Treatment of Impairments:
Shankhpushpi:
Shankh-pushpi, a popular Ayurvedic drug, is used for a number of CNS effects, most notably memory enhancement. It is unclear where the term "shankhpushpi" originated because it is used to refer to a number of plants in different locations of India. Plants commonly referred to as shankhpushpi include Convolvulus pluricaulis Chois., Evolvulus alsinoides Linn., and Clitoria ternatea Linn. (Leguminosae).[33]
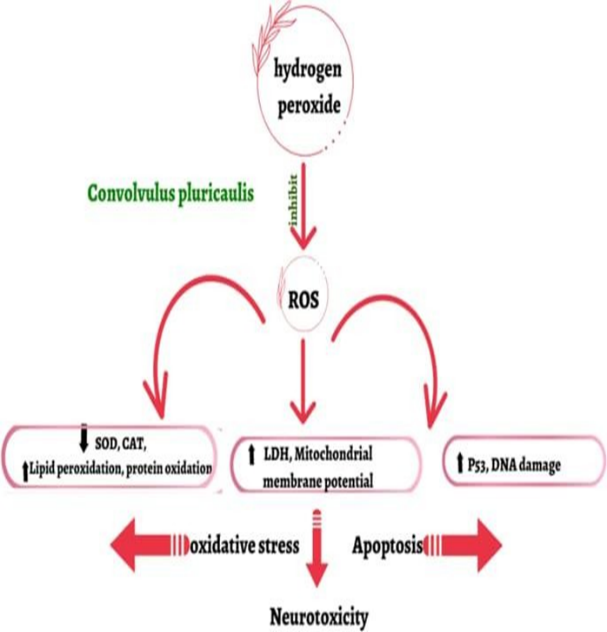
Shankhpushpi (Convolvulus pluricaulis) is an Ayurvedic cognitive enhancer (nootropic) that regulates neurotransmitters, shields brain cells, and enhances learning, memory, focus, and stress/anxiety. It is applied as a "brain tonic" to improve overall mental clarity and cognitive function

(Fig. – 3.1 Flowers of Shankhpushpi)
Botanical Description:
Shankhpushpi, mostly Convolvulus pluricaulis, is a prostrate, perennial herb belonging to the Convolvulaceae family. It is distinguished by its hairy, spreading branches, short, arrowhead-shaped leaves, and characteristic conch-shaped blooms that appear in the morning. Its slender roots, bitter taste, and cold strength make it an Ayurvedic brain tonic. The entire plant is used as a natural sedative and for memory, stress alleviation, and Pitta/Kapha dosha balance.
Plant Characteristics:
Chemical Constituents:
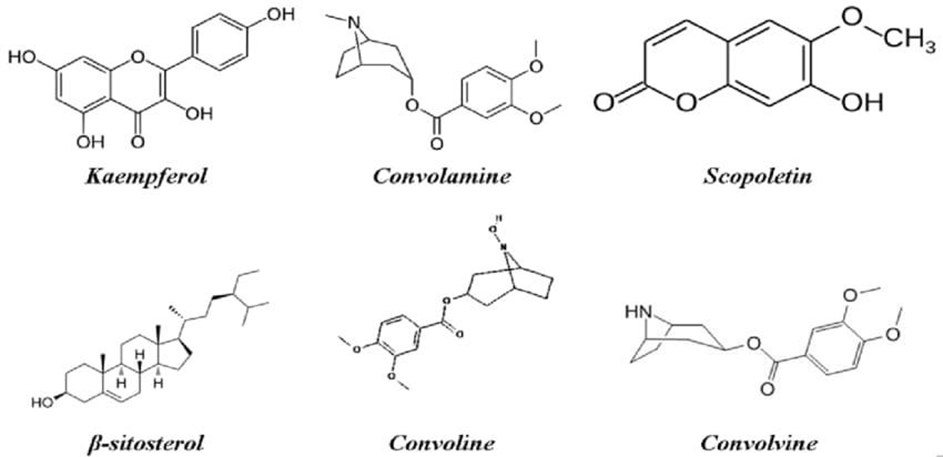
The mystical herbal remedy has a number of active substances, including alkaloids like convolvuline, convolidine, convolvine, convolamine, convoline, confoline, and convozine.
Additionally found are volatile oils, fatty acids, fatty alcohols, hydrocarbons, palmitic acids, linoleic acids, myristic acids, flavonoids, steroids-phytosterols, D-glucose, maltose, sucrose, starch, rhamnose, and other carbs, proteins, and amino acids.
Therapeutical Uses:
Mentha:
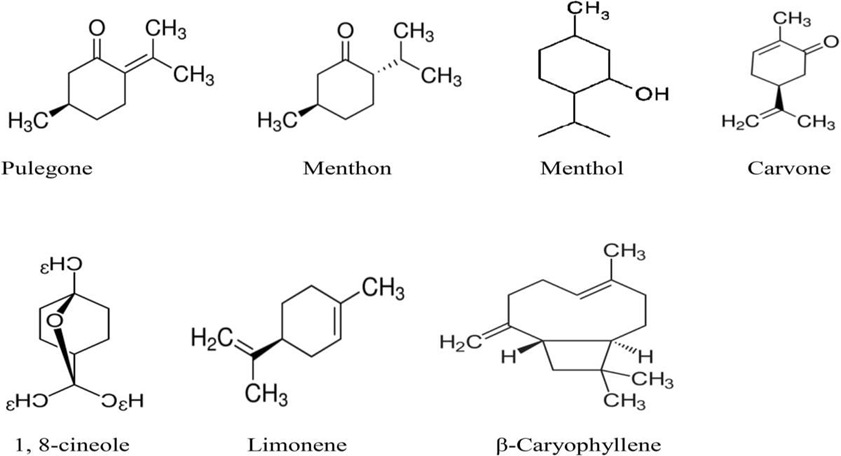
Mentha, or mint, primarily enhances attention, memory, and alertness while reducing mental fatigue through its effects on neurotransmitter systems (cholinergic, GABAergic) and increased brain wave activity. Studies have demonstrated that peppermint (Mentha piperita) and spearmint (Mentha spicata) extracts or essential oils improve mood and vigor as well as performance on challenging tasks.The main chemical groups responsible for Mentha's diverse range of bioactivities are believed to be polyphenols and essential oils (EO). The EO of Mentha includes terpenoids, menthol, menthone, neomenthol, menthyl acetate, isomenthone, 1,8-cineole, linalool, α-pinene, β-pinene, limonene, carvone, and pulegone, as well as monoterpenes and sesquiterpenes, the quantity of which varies from species to species.[34]

(Fig. – 3.2 Leaves of Mentha)
Botanical Description:
Mint (Genus Mentha) is a fragrant, square-stemmed perennial herb belonging to the Lamiaceae family. It spreads quickly through underground rhizomes and stolons (runners) and is characterized by opposing, serrated leaves with tiny oil glands and small, frequently purplish flowers in whorled clusters (verticillasters). Its various varieties and hybrids differ in height (4-120 cm), leaf form (oblong to lanceolate), and blossom color (white to purple). Other important characteristics are fragrant leaves, square stems, and opposing leaves.
Plant Characteristics:
Chemical Constituents:
It belongs to the Lamiaceae family. Menthol demonstrated its antioxidant activity by raising the activities of the GSH antioxidant and the enzymes GSH-Px and GR in the menthol-treated group compared to the vehicle-treated group. Menthol showed immunomodulatory properties; in stomach tissue, it reduced the pro-inflammatory cytokines TNF and IL-6 and elevated the anti-inflammatory cytokine IL-1.[35]
The capacity of mentha, often known as mint, to enhance cognitive performance is supported by a variety of chemical components. Among the crucial materials are:
Therapeutical Uses:
Liquorice:
Licorice (Glycyrrhiza glabra) contains anti-inflammatory and antioxidant chemicals called glycyrrhizin, which may improve memory and learning while protecting against oxidative stress and neuroinflammation linked to conditions including depression, Alzheimer's, and stroke. It may enhance memory by reducing inflammatory cytokines and raising brain-derived neurotrophic factor (BDNF); nevertheless, high dosages may have negative consequences that warrant caution.

(Fig. – 3.3 Dried root of Liquorice )
Botanical Description:
Growing up to 1-2 meters tall, licorice (Glycyrrhiza glabra) is a perennial herb in the pea family (Leguminosae) that is distinguished by its large root system and sweet, woody root with a bright yellow interior. It produces spikes of tiny, pea-like blooms that are white, pale blue, or purple, followed by flattened seed pods. Its pinnate leaves have nine to seventeen leaflets. The root, which is harvested after a number of years for its sweet extract used in food and medicinal, is the main beneficial part
Plant Characteristics:
Phyto-Chemical Constituents:
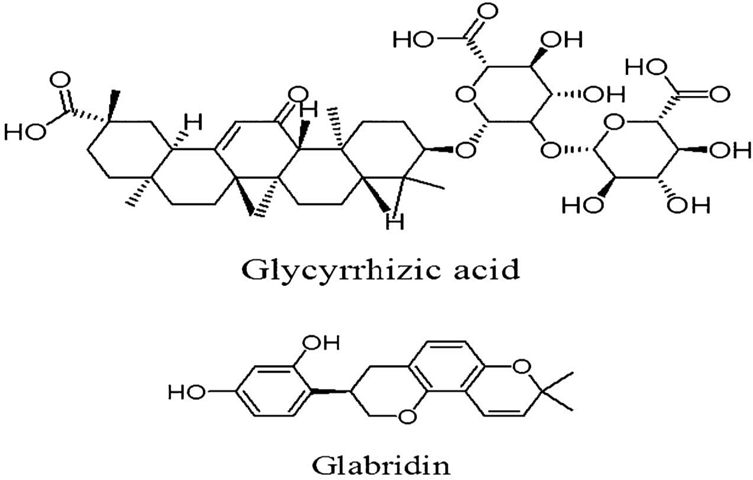
The sweet triterpenoid saponin glycyrrhizin (also called glycyrrhizic acid) and several flavonoids are the main active compounds found in liquorice root, along with sugars, polysaccharides, starches, and minerals. These compounds give liquorice root its sweet flavor and a range of pharmacological effects, such as anti-inflammatory and antioxidant properties. There are more than 400 known phytochemicals.
Therapeutical Uses:
Licorice, or Glycyrrhiza glabra, has a number of therapeutic uses that can enhance cognitive performance. Here are some of its primary benefits:
CONCLUSION
The nootropic mixture made with Shankhpushpi, mint, and licorice has encouraging potential for enhancing cognitive abilities like learning, memory, and mental alertness. Mint helps to promote focus and mental clarity, while Shankhpushpi is well known for its neuroprotective and memory-boosting qualities. Licorice has antioxidant and adaptogenic properties that enhance general brain health and lessen mental stress. The combination formulation may work in concert to preserve normal neuronal function and improve cognitive performance. Compared to synthetic nootropic drugs, this formulation is anticipated to provide superior safety and tolerability due to its herbal composition. However, additional pharmacological testing, standardization, and clinical research are needed to confirm its safety and effectiveness. The results support the traditional usage of Shankhpushpi for its neuropharmacological activity and offer significant implications for its application in the treatment and prevention of memory and CNS-related disorders. E. alsinoides is a promising agent for controlled clinical trials to determine its safety and efficacy as an antioxidant, NSAID-like prophylactic agent, NMDA down-regulator, and acetylcholinesterase enhancer for protection against AD and possibly other neurodegenerative age-related diseases due to its comparative multiple beneficial effects over other Shankhpushpi botanicals. Neuropharmacological activity data indicate that while the other three plants can be utilized as Shankhpushpi substitutes, E. alsinoides should be the actual source
REFERENCES
https://doi.org/10.1146/annurev.neuro.29.051605.112819, 2-s2.0-33748361335.
[Google Scholar]
[PubMed] [Google Scholar]
effects of anti-dementia and nootropic treatments on the mortality of patients with dementia: A population-based cohort study in Taiwan. PLoS ONE. 2015;10:e0130993. doi: 10.1371/journal.pone.0130993. [DOI] [PMC free article] [PubMed] [Google Scholar]
J. Herb. Med. 2010;22:64–65. [Google Scholar]
[PubMed] [Google Scholar]
[Google Scholar]
312. doi: 10.2165/11319230-000000000-00000. [DOI] [PubMed] [Google Scholar]
https://doi.org/10.1146/annurev.neuro.29.051605.112819, 2-s2.0-33748361335.
[Google Scholar]
[PubMed] [Google Scholar]
effects of anti-dementia and nootropic treatments on the mortality of patients with dementia: A population-based cohort study in Taiwan. PLoS ONE. 2015;10:e0130993. doi: 10.1371/journal.pone.0130993. [DOI] [PMC free article] [PubMed] [Google Scholar]
J. Herb. Med. 2010;22:64–65. [Google Scholar]
[PubMed] [Google Scholar]
[Google Scholar]
312. doi: 10.2165/11319230-000000000-00000. [DOI] [PubMed] [Google Scholar]

Chanchal Sahu, Shweta Ram, Dr. Gyanesh Sahu, Suchita Wamankar, Neuroprotective and Nootropic Potential of Shankhpushpi (Convolvulus Pluricaulis) And Its Polyherbal Formulations in Stress-Induced Cognitive Impairment: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 934-950. https://doi.org/10.5281/zenodo.18934248
 10.5281/zenodo.18934248
10.5281/zenodo.18934248