
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens College of Pharmacy, Peth Vadgaon, Maharashtra, India
Microneedle drug delivery system is an effective approach for the delivery of the drugs by the transdermal route. The microneedles create the micro sized pores on the skin surface and the drug enters to the dermis through cuticle layer. Stratum corneum is a barrier of skin, sclera and cornea that challenges the topical administration of the drugs and entry of the exogenous materials. Also, for transdermal delivery the drug should obey specific physicochemical properties like, the drug should have a molecular size less than 500 D, it should have a low melting point, as well as adequate lipophilicity. Ideally log P should be within 2-3. Thus the drugs which are hydrophilic in nature, or macromolecular agents like proteins, peptides, DNA, small interfering RNA, etc. are difficult to administer via transdermal route. Therefore, microneedle system can be incorporated to increase the drug permeation through subcutaneous layer. It also bypasses the hepatic circulation and first pass metabolism, increasing the bioavailability of the drugs. In this review article we have discussed about the microneedle drug delivery system including its types, applications, and newer approaches in the field of microneedles.
One of the most practical ways to administer medications is orally however occasionally this is not possible since medications may be poorly absorbed or destroyed as a result of enzymatic breakdown in the liver or gastrointestinal tract over the past century injection using a hypodermic needle has become a popular substitute for oral drug delivery which are more painful and invasive also create the biohazardous waste and require trained personnel Hypodermic needles are inserted to muscles where there is a lower immune response than there in the skin so TDDS is used as an alternative method to the hypodermic needles TDDS also bypasses the hepatic first pass metabolism and it is non-invasive painless alternative and it can be self-administered stratum corneum is the outermost layer of the skin made up of the dead corneocytes that acts as a primary barrier for transdermal administration it causes significantly reduced effectiveness of the drug delivery and restricts the different kinds of the drugs that are transported via skin Microneedle technology was proposed in year 1976 to overcome the problems associated with old transdermal delivery technique The microneedles are about 25 um to 2000um long and are much sharper than the usual hypodermic needles so that they can cross stratum corneum and create micro scale drug delivery channels without disturbing the nerve fibers and blood vessels present in the epidermis and dermis layers of the skin therefore the efficacy of the drug delivery can be markedly improved and a wide range of drugs delivered by TDDS can be significantly expanded in a painless and least invasive way.
2. CLASSIFICATION OF MICRONEEDLES:
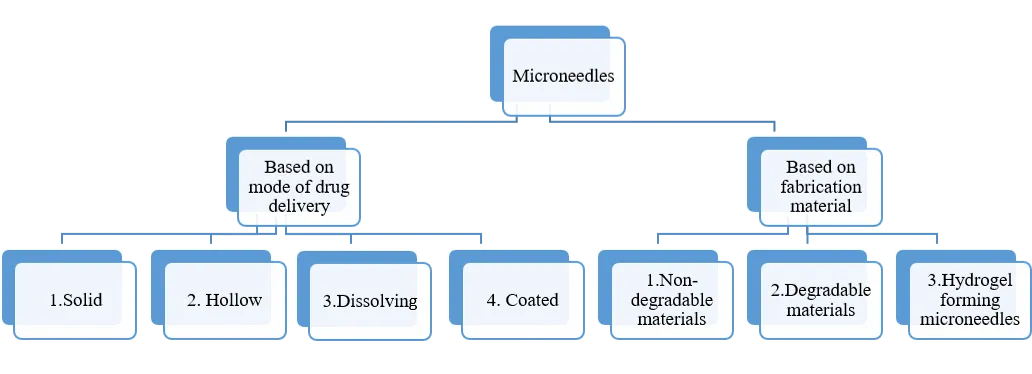
Figure 1: Classification of microneedles
2.1 Based on mode of drug delivery:
There are four types of microneedles: Solid, hollow, dissolving and coated microneedles.
2.1.1 Solids microneedles:
Since solid microneedles are introduced and removed to create pores on the skin’s surface that are micro in size, they can be utilized in the skin pre-treatments They function by creating micro channels using the “poke and patch” method. These micro channels increase the permeability of the medication by permitting diffusion straight into the dermal layer from a formulation. An experiments on rat skin has demonstrated that when placed under occlusive conditions such as occlusive tape, the micro pores created by the microneedles persisted for at least 72 hours following microneedle therapy. Without applying occlusive tape, the micro pores quickly closed. It was found that the solid MN-created micro channels healed quickly in just 2 hours, without causing secondary infection. The “scrape and patch” method is modification of the standard solid microneedle technique in which microneedle, micro projections, or micro blades are scraped over the skin to create micro-abrasions. These microprojection are subsequently covered with drug solution in patch. An additional alternative is to utilize a roller with solid microneedles that repeatedly puncture the stratum corneum as the roller rotates across the skin pores. A study by Ita et al (2015) used Microneedle Systems with a cylindrical surface to administer medications for high blood pressure. Transdermal flow values have been observed to rise 5-6 times following microneedle roller treatment using pig skin.
2.1.2 Hollow microneedles:
The microneedles are a tiny version of the traditional hypodermic needle systems. A pressure-driven liquid formulation flow is used to administer drugs. This method can deliver significant dosages into the dermal layer. It is challenging to construct hollow microneedles because of their fragility and structure. The hollow microneedle work on the principle of ‘puncture & flow’. Davis et al (2005) created a series of hollow metal microneedles for one such study. In diabetic rats, the administration of insulin using these microneedles was investigated. The study found that the pharmacodynamics profiles of hollow microneedles are similar to those of a conventional hypodermic injection.
2.1.3 Dissolving microneedles:
These types of microneedles are governed by “poke & release” principle. Compared to other microneedles, they are simple to use and manufacture, which is why they have attracted a lot of interest recently. The biodegradable elements used to make dissolving Microneedles include sugars and biodegradable polymers loaded with medical compounds. The conjugated therapeutic agent is released when the microneedles dissolve into the skin after applications. Because of their single-step application approach and ease of manufacture, these microneedles offer an advantage over convenient. Microarrays made of dissolving hyaluronic acid were created by Liu et al. When used as microneedle array, the cumulative penetrated amount of dextran rose by an astonishing 610 times with minimal lag drug penetration time. Researchers are looking into using dissolving microneedles to deliver vaccines via the skin. It has been demonstrated that carboxy methyl cellulose and hyaluronan microneedle totally disintegrate in rat skin, 5minutes after applications, releasing the IgG payload specific to the antigen.
2.1.4 Coated microneedles:
Coated microneedles are those that operate on the “coat and poke” principle. These microneedles are made out of a solid microneedle foundation covered in medication solutions or dispersions. Numerous studies have been investigated for coating microneedles. Dip coating is the most used technique, but it is challenging because it requires exact control to ensure that the microneedles are introduced into the dipping solution precisely. Another technique for drug deposition on microneedles is spray coating; however, this approach is unable to prevent drug loss due to spraying on the array of microneedles’ substrate, which is inaccessible for drug penetration.
Although aerosol coating techniques are more effective, the usage of thermolabile medications may be restricted due to the requirement for temperatures as high as 200°C. Ma et al (2018) used a polyethylene glycol matrix to cover solid microneedles with suspended lidocaine that demonstrated a noticeably greater delivery than marketed product. Since they provide a comparatively modest surface area for medication absorption, coated microneedles are employed less frequently than other microneedles.
Following is a comprehensive overview of the benefits, drawbacks, and mode of drug delivery of different microneedles:
Table 1 : An overview of microneedles
|
Type of microneedles |
Benefits |
Drawbacks |
Mode of drug delivery |
|
Solid microneedles |
These can be fabricated with different types of materials |
1.Can break beneath the dermal layers. 2.Minimum surface area for drug absorption |
By making micropores to the skin through which the drug is delivered |
|
Hollow Microneedles |
High doses of drugs can be delivered |
Require a strong material of manufacturing to resist flow pressure. |
Pressure driven flow through the needles |
|
Dissolving microneedles |
Simple manufacturing |
Can be made up of only biodegradable substances |
Dissolves beneath skin to release drug payload |
|
Coated microneedles |
Potent drugs requiring low dose can be delivered |
1.Drug loss during fabrication 2.Temperature control is required |
Drug is released through the coating |
2.2 Based on fabrication material:
Microneedles are manufactured using a various types of material including metals, ceramics, silicones, and polymers. These materials used for microneedles manufacture are classified as non- degradable and degradable materials. Materials such as metals, ceramics and silicones are non- degradable materials while the polysaccharides and polymers are the degradable materials that are employed in microneedle manufacturing.
2.2.1 Non degradable materials:
2.2.2 Degradable materials:
Microneedles have been made from a variety of materials. They can be made from either biodegradable or non-biodegradable materials. Although there are many options for both biodegradable and non-biodegradable materials, it is important to take into account supporting factors that may affect the building materials. Several types of materials have been used for fabrication of microneedles. The choice of material is influenced by a number of factors, including the available manufacturing method, the drugs and excipients of choice, the drug’s compatibility with the material and fabrication process, the eventual usage, and the mode of delivery.
3. FABRICATION TECHNIQUES OF MICRONEEDLES:
Skin is an elastic organ that has considerablevtensile strength. Microneedles need to be as strong as possible to penetrate without breaking or cracking during insertion. As a result, creating microneedles is difficult. The required skin depth, microneedles geometry, and preferred material all influence the construction process. For example, solvent- casting might work well for polymeric microneedles, whereas metal microneedles are best designed using microelectromechanical system. The manufacturing technology has been used to categorize the fabrication procedures.
(i) Deposition, (ii) patterning, and (iii) etching.
This process involves the creation of films on substrate, which is a base material. A chemical or physical process creates the films. While the chemical vapour deposition (CVD) technique involves a chemical reaction between the hot substrate and the carrier gases in the chamber, the physical vapour deposition (PVD) technique involves removing the materials from the source and depositing them on the substrate.
The microneedle geometry pattern, such as height, base width, tip angle, and bore size details is transferred onto the film during the patterning process. One popular method for patterning is lithography. In short, a microneedle pattern is transferred when a radiation source, like light strikes a photosensitive substrate. Radiation can come from a variety of sources, including x-ray, ion, or electron beam lithography. The mask transfer onto the photosensitive coated substrate typically involves the following successive steps:
The first stage is heating in the presence of steam or humidified oxygen to generate an oxide layer. A thin layer of an organic polymer known as a photosensitive/ photoresist or resist substances (sensitive to UV radiation) is then spin coated. The resist layer is then heated in order to eliminate the solvent. After that a mask is exposed to a UV lamp, which enables an almost flawless transfer or to put it another way, ‘printing’ of the mask image onto the resist-coated wafers.
In order to create an interesting microneedle design, the unprotected portions of the substrate are etched out using a strong caustic solution. Both wet and dry methods can be used for etching.
When compared to hypodermic needles, microneedles have a significant benefit in terms of pain. Microneedles’ number has a minor impact on pain, whereas microneedles’ length has a greater influence. Microneedles that are less than 400µm often cause little pain. Pain for hollow microneedles diminishes with reduced flow and hyaluronidase use, but increases with increased pressure and flow rate. In general, microneedles are painless, and their design is not significantly hampered by discomfort.
4. APPLICATIONS OF MICRONEEDLES:
In contrast to traditional patches, microneedle systems frequently need outside help to penetrate biological tissues consistently and reliably. While applicator devices allow for consistent microneedle insertion with less inter-individual variability, manual application may result in varying insertion depth and applied pressure. Microneedle arrays provide regulated penetration into stratum corneum and can be applied to the skin before device is activated or pre-mounted with applicator. Both single use and multiple use setups are supported by reported applicator design.
The ability of a molecule to enter the skin is a major factor in the effectiveness of transdermal medication delivery. Due to their enormous molecular size, many compounds particularly peptides and vaccines have faced challenges during formulation and application. When compared to traditional delivery methods, microneedles have shown efficacy in delivering these molecules intradermally and, in certain instances, have been able to achieve the same therapeutic impact at lower doses. For instance, employing microneedles rather than conventional intramuscular administration resulted in a similar increase in hemagglutinin inhibition antibody titer with less than half the medication dose.
Several regulatory bodies have approved microneedle devices for the delivery of seasonal influenza vaccinations, further demonstrating their efficacy. Microneedles have also been investigated for the treatment of psoriasis, dermatitis, viral warts, and even skin cancer. Microneedles are being studied for ocular medication administration in addition to intradermal applications, and they have shown encouraging outcomes in the treatment of disorders such glaucoma, macular degeneration, uveitis, and retinal vascular occlusion. Currently, the majority of commercially available microneedles are used in cosmetic applications; dissolving microneedles are frequently used to treat acne, while dermarollers improve the general health of the skin.
Yun Liu et al described various applications of polymeric microneedles as follows:
Insulin delivery devises, which are known for their rapid in vivo glucose responsiveness, usually have limited insulin carrying capacity and pose manufacturing issues. Therefore, the rapid in vivo glucose release response seen in pancreatic β-cells is being replicated in microneedle devices for blood glucose management, while also emphasizing excellent biocompatibility to address acute and long term toxicity concerns. By avoiding the epidermal barrier and enabling the direct administration of macromolecules using a variety of microneedles, the microneedle patch provides a clear advantage. This characteristic increases their effectiveness in reducing pain, making them favoured choice for people with long term medical conditions like diabetes tat requires ongoing treatment. Dopamine nanoparticles (PDA NPs) are incorporated into the exterior layer of microneedle system in a unique method devised by Ma and colleagues. By improving the microneedles’ adherence to skin tissue, this design helps diabeteic wounds heal more quickly. Synthetic nanovescicles ( NV) generated from mesenchymal stem cells (MSCs) are produced by extrusion via a porous membrane showed significant improvements in mRNA and protein expression levels, as well as a noteworthy 250- fold increase in manufacturing yield. The PDA microneedle patch’s powerful therapeutic growth factor offers significant benefits in boosting collagen regeneration, decreasing inflammation, and encouraging angiogenesis. Additionally, the potential benefits of polymeric microneedles medication delivery devices for wound healing management were shown.
The medicine can reach the stimulation site and the associated subcutaneous tissues and be quickly dissolved or destroyed with excellent bioavailability thanks to the microneedle drug delivery system, which completely encapsulates the drug within the microarrays. One of the most successful medication delivery techniques for skin cancer and other cancer treatments is microneedling. Compared to conventional metal and glass micro and nanomaterials, polymer- based micro and nanocomposited provide benefits such as high drug loading, structural durability, and the elimination of the requirement for external drug storage. The very hydrophobic and biocompatible polycaprolactone (PCL) enhaces the solubility and bioavailability of low molecular weight lipid soluble medications.
Drugs are delivered at a more effective drug release rate using a hydrophilic crosslinked PVP polymer microneedle device. In the 500 µg/mL concentration range, PCL and PNVP are both highly biodegradable and non-toxic, which enhances the effectiveness of low molecular weight drug delivery and guarantees long-term safety. Additionally, both of them work well with blood, which facilitate the systematic distribution of medications. The polymer based hydrogel made from carboxy methyl cellulose can mimic the pharmacokinetic process of cellular DOX release in vivo, hence enhancing the therapy of melanoma cancer cells. Polymer microneedles insertion site’s long term durability guarantees the steady blood pressure and long lasting pharmacological benefits that improve performance and lower the risk of infection. In conclusion, compared to traditional drug release techniques, polymer microneedle architectures exhibit significant potential for enhancing drug bioavailability, extending circulation time, regulating drug release and tumor targeting.
In order to avoid systemic toxicity or infection, the long term management of chronic pain restricts the use of delivery methods like parenteral injections. Treatment resistance brought on by patient’s skin nociceptive sensitivity to pain is effectively reduced by microneedle device reacts to biophysical cues gathered in subcutaneous tissue for potential physiological monitoring in case of secondary pain brought on by complex disorders like diabetes.
Therapeutic agents must be delivered locally and specifically to treat problems connected to chronic pain. For the treatment of chronic pain, transdermal delivery devices such as microneedles offer a slow- release mechanism that guarantees sustained plasma delivery and medication efficacy. The microneedle administration devices prevented substance misuse and dramatically decreases the frequency of treatment programs for managing chronic pain. The physicochemical characteristics of the medication (such as solubility, partition coefficient, hydrophobicity), loading dose, molecular diffusivity, and polymer layer all affect the therapeutic efficacy of traditional transdermal patches. Although oral meloxicam effectively reduces osteoarthritis pain in individuals, it has side effects such as ulceration and perforation.
Currently, corticosteroids, non-steroidal anti-inflammatory agents (NSAIDs), and disease modifying antirheumatic drugs (DMARDs) including Etanercept and methotrexate are the main treatments for rheumatoid arthritis. These drugs are often administered orally or by subcutaneous and intramuscular injections. A viable alternative for transdermal drug delivery is microneedle arrays, which may avoid first pass metabolism and its dangerous side effects, including hepatotoxicity, myelosuppression and gastrointestinal bleeding. Compared to traditional delivery methods, this strategy also reduces the risk of infection and improves patient compliance.
Drug delivery vehicles are made of nanoscale synthetic and natural polymers with diameters under 200 mm. These polymers encapsulation of therapeutic substances enables tailored administration to inflammatory areas, encouraging localized drug accumulation and reducing medication waste overall. According to a new study, delivering antigens to antigen presenting cells (APCs) via polymer microneedles promotes a crucial interaction with antigen specific CD4+T cells. Significant anti-inflammatory qualities are conferred with a living organism by this interaction, which successfully controls T cell development into regulatory T cells. Its therapeutic potential has been demonstrated by a notable reduction in the anti-inflammatory response. Additionally, a variety of therapeutic agents, such as genes, nucleic acids and antigen-specific modified cells and proteins, can be delivered more easily. For rheumatoid arthritis, microneedle system offers a very promising substitute for traditional drug delivery techniques, with the possibility for affordable, secure, and long lasting therapeutic treatments.
The most effective method of controlling infectious diseases is preventive vaccination, and the way is administered is crucial to its effectiveness. An important development that offers a viable substitute for the conventional approaches is the introduction of microneedle system-based vaccination administration. The need for cryogenic storage and transportation, which limits accessibility, is a significant obstacle in the delivery of the BCG vaccination. This invention offers a potential remedy for the cold-chain dependency by preserving the vaccine’s immunogenicity and antigenic qualities without sacrificing its efficacy or integrity.
While significantly preventing skin irritation and the development of post-vaccination scars, the BCG vaccine administered using microneedle powder (BCG-MNP) shows efficacy comparable to the conventional intradermal delivery. By effectively introducing antigens to the skin’s dendritic cells (DCs), this microneedle-based vaccination approach produces a strong local immune response that is not seen with intramuscular injections. The choice of microneedle matrix biomaterials is important since they can enhance the immune response and modify the vaccine’s immunogenicity.
5. CONCLUSION:
By successfully getting over the stratum corneum barrier, microneedle-based medication delivery systems mark a substantial breakthrough in the field of transdermal therapies. Microneedles provide a less intrusive, painless, and patient-friendly option with better bioavailability and fewer systemic side effects than traditional delivery methods like oral administration and hypodermic injections.
Depending on the therapeutic need, a variety of microneedle types, such as solid, hollow, dissolving, and coated systems, offer flexible platforms for drug administration. Additionally, the development of microneedles with improved mechanical strength, accuracy, and drug-loading capacity has been made possible by the variety of fabrication materials and sophisticated production procedures.
Microneedles have a wide range of therapeutic applications, including vaccine administration, diabetes management, cancer therapy, pain management, and dermatological diseases. Notwithstanding these encouraging benefits, issues with cost-effectiveness, long-term safety, regulatory approval, and large-scale manufacturing still need to be resolved.
All things considered, microneedle technology has enormous potential as a cutting-edge medication delivery method that could transform contemporary treatments and enhance patient compliance.
6. FUTURE OUTLOOK:
Microneedle drug delivery systems have a bright future thanks to continuous developments in biomedical engineering, materials science, and microfabrication technologies. It is anticipated that new techniques such hydrogel-forming systems, stimuli-responsive drug delivery platforms, and smart microneedles would further improve therapeutic accuracy and efficiency. Personalized medicine may be made possible by the integration of microneedles with digital health technology, such as wearables and biosensors, which could allow for regulated drug delivery and real-time monitoring. Furthermore, the creation of self-administrable microneedle patches has the potential to greatly increase healthcare accessibility, particularly in environments with low resources.
Since microneedles reduce the requirement for cold-chain storage and skilled staff, more study is also expected in the field of vaccine delivery, especially for quick immunization during pandemics. It is anticipated that developments in 3D printing and additive manufacturing would enable affordable mass production and customizable designs.
Future research, however, must concentrate on guaranteeing long-term safety, drug formulation stability, regulatory consistency, and patient acceptance in order to achieve broad clinical adoption. Microneedle technologies have the potential to be a key component of targeted and non-invasive medication delivery in the future with further development and interdisciplinary cooperation.
REFERENCES

Srushti Devkule, Shruti Patil, Vaishnavi Mane, Lija Mujawar, Sindhu Shedbale, Dhanraj Jadge, A Review on Microneedle Drug Delivery Systems: Classification, Fabrication, and Biomedical Applications, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 81-96. https://doi.org/10.5281/zenodo.20483349
 10.5281/zenodo.20483349
10.5281/zenodo.20483349