
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Swami Vivekanand College of Pharmacy, Udgir
A Transdermal patch is a medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the bloodstream. The transdermal drug delivery system is one of the novel drug delivery systems which overcome arise from the conventional dosage. Transdermal patches are pharmaceutical preparation of varying sizes, containing one or more active ingredients to the systemic circulations. The review gives valuable information about the transdermal patch like its advantage, disadvantage, mechanism of action, types of transdermal patch, factors basic components, methods and evaluation, application of a transdermal patch. A wide variety of pharmaceuticals are now available in transdermal patch form.
Transdermal drug delivery systems often referred to as "patches," represent pharmaceutical formulations meticulously crafted to transport a clinically beneficial quantity of medication through a patient's skin. To accomplish the task of conveying therapeutic agents across human skin for systemic impact, it is imperative to thoroughly evaluate the skin's intricate morphological, biophysical, and physicochemical attributes.
Transdermal medication is available for controlling and treating various condition such as hypertension, rheumatoid arthritis, diabetes mellitus, psychiatry disorder, motion sickness, migraine, neurological disorder, smoking cessation. Transdermal device offers a painless technique of discrete self-controlled delivery of medication into the blood stream for various body and skin related issues over a prolong period. to sustain the objective, the drug release from transdermal patches may follow zero or first order kinetic. Zero order kinetic is constant release kinetic means the drug released from patch at a constant rate over time. First order kinetic refers to a drug release profile where the concentration decreases exponentially overtime. Transdermal patch has proven to be a valuable tool in expanding the application of existing therapeutics and addressing the limitations of first pass drug degradation, this metabolism can significantly reduce the bioavailability of orally administered drug.
Oestradiol patches are a commonly used form of medication, with over a million patients using them annually. Unlike the oral formulation of oestradiol, these patches do not cause liver damage. Apart from therapeutic oestradiol patches, there are also two major subcategories of patches available in the market: aroma patches and non-medicated patches. Aroma patches are typically used for their fragrance or therapeutic properties. Non medicated patches include a wide range of product, such as thermal and cold patches, nutrient patches, and skin care patches.
A transdermal drug delivery system (TDDS) often referred to as "patches". It is a pharmaceutical technology designed to administer medication through the skin for systemic distribution in the body. Transdermal drug delivery systems optimize treatment by modifying pharmacokinetic parameters, releasing drugs through zero order kinetics, first order kinetics, or both.[1]
2. TDDS PATCH DESIGN: -
Transportation of drug across the skin is affected by various factors, such as skin permeability, area, and duration of application, as well as metabolic activity of the skin (i.e., first pass metabolism). In fact, every drug has its unique properties, which can affect transdermal delivery. To achieve adequate skin absorption and penetration, the drug should
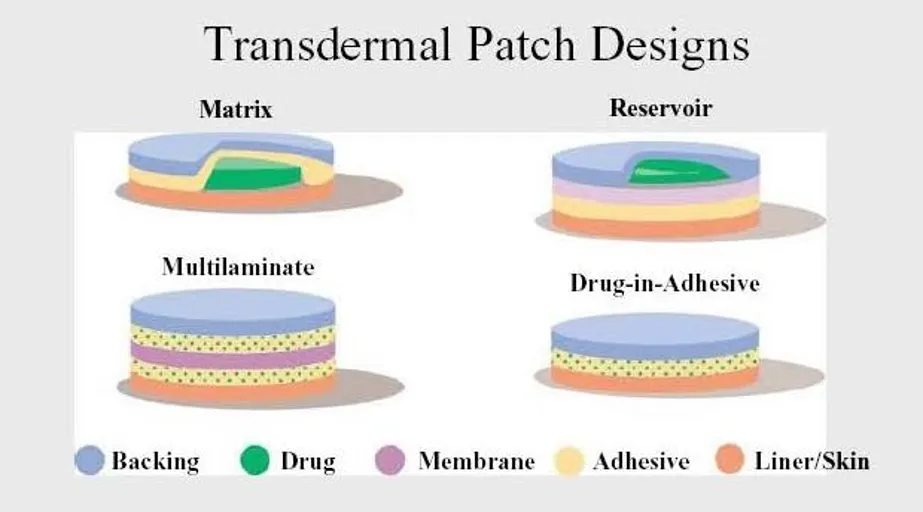
Figure 1 Transdermal Patch Design
be non-ionic and relatively lipophilic to cross the skin barrier. Molecules larger than 500 Daltons make it difficult to cross the stratum corneum, and ideally the therapeutic dose of the drug should also be less than 10 mg per day.[2]
Basic Component of Transdermal Patch Transdermal patches typically consist of several layers that are designed to deliver the medication through the skin and into the bloodstream. Figure 1 illustrates the basic component of a medicated patch. The specific composition and structure of the patch may vary depending on the drug being delivered and the desired rate of drug release.
The backing layer is the outermost layer of the patch and serves to protect the other layers from the environment. This layer is usually made of a flexible, waterproof material such as polyethylene or polypropylene. The adhesive layer serves to attach the patch to the skin and keep it in place. It usually consists of a strong, hypoallergenic adhesive that is gentle on the skin. The drug layer contains drugs that are delivered through the skin. It is formulated to release the drugs at a constant rate over a period. The rate-controlling membrane serves to control the rate at which the drugs are released from the patch. Membranes are usually made of semi-permeable materials that allow the drugs to pass through the membrane at a controlled rate. Linen acts as a protector for the patch and adhesive. The patch must be removed before being applied to the skin surface.[2]
3. TYPES OF TDDS PATCHES: -
3.1 Single Layer Drug-in-adhesive Patches
A single-layer drug-in-adhesive (DIA) patch is a type of transdermal drug delivery system in which the drug is directly incorporated into the skin-contacting adhesive layer. In this design, the adhesive layer serves multiple functions it acts as the drug reservoir, ensures the patch adheres to the skin, and enables drug release by diffusion through the skin. Above this adhesive-drug layer is an impermeable backing membrane that protects the patch and drug from environmental exposure (moisture, oxygen, etc.), and below (or rather before application) there is a release liner which is removed before the patch is applied to skin. Thus, the entire formulation (drug + adhesive + excipients) is confined within a single adhesive layer under one backing film. When the patch is applied, the drug diffuses from the adhesive into the stratum corneum and then onward into systemic circulation, delivering a controlled dose. This design is relatively simple compared to multilayer or reservoir systems. It is often suitable for potent drugs that require low-dose continuous delivery, and for drugs whose physicochemical properties (lipid solubility, molecular weight, skin permeability) make them amenable to transdermal diffusion. Because of its simplicity, single-layer DIA patches are generally easier to manufacture and more cost-effective; their patch thickness tends to be low, making them more comfortable for patients. However, drug loading capacity is limited, so only drugs requiring relatively low therapeutic doses are ideal. Also, release rate depends largely on drug diffusion through skin, which can be influenced by skin condition, adhesive properties, and formulation factors.[3]
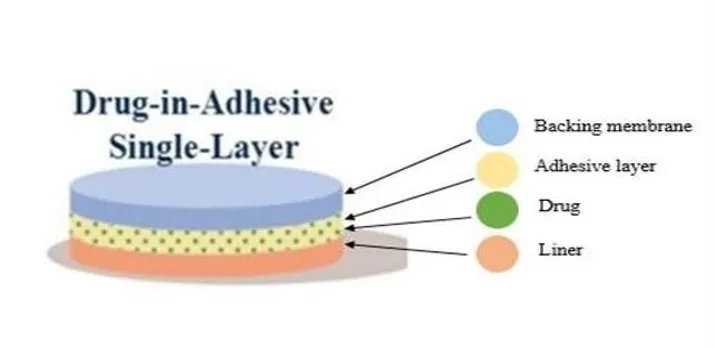
Figure 2 Single Layer Drug-in-adhesive Patches
3.2 Multilayer Drug-in-adhesive Patches [4]
A multilayer drug-in-adhesive (DIA) patch is a transdermal system in which multiple adhesive layers each potentially containing drug - are stacked under a single backing film, in contrast to a single-layer patch which has only one adhesive layer containing the drug. In a multilayer design, one layer may be formulated for immediate/initial drug release, while another layer provides sustained or controlled release. Sometimes a thin membrane printer-adhesive liner may separate these layers to modulate diffusion or to prevent mixing, thereby allowing a more refined control over release kinetics. Underneath the adhesive layers sits an I am prebaking membrane that protects the patch contents; a removable release liner covers the adhesive before application. When applied to skin, drugs diffuse froth drug-loaded adhesive layers, layer by layer, through the skin's stratum corneum into systemic circulation. This arrangement enables a biphasic or multi-phase release profile: an initial "burst" dose from the first adhesive layer followed by a steady maintenance dose from deeper layers. Such a system improves therapeutic flexibility, allowing adjustment of dosage and release kinetics. It is particularly useful for drugs that require a loading dose followed by sustained therapeutic levels, or when combining multiple drugs requiring different release patterns. Multilayer DIA patches also offer advantages like higher overall drug loading compared to single-layer patches (since there are multiple adhesive strata), improved adhesion and patch stability, and reduced risk of premature dose dumping. However, designing multilayer patches is more complex - formulators must carefully optimize adhesive types, drug concentration per layer, inter-layer compatibility, and membrane/liner placement to ensure uniform release. Also, skin irritation risk, adhesive strength, and manufacturing reproducibility require thorough validation days.
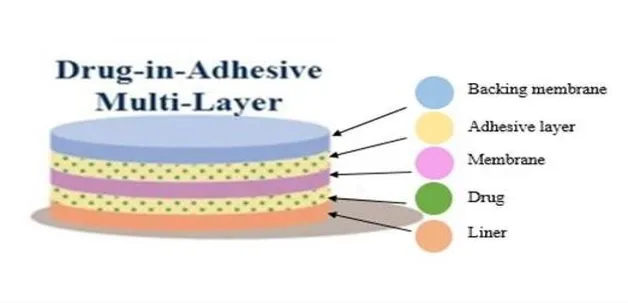
Figure 3 Multilayer Drug-in-adhesive Patches
3.3 Vapor Transdermal Patches [4]
Vapour transdermal patches are a type of adhesive patch designed to release vapours, often from essential oils or other volatile compounds, onto the skin over time, providing localized systemic effects.
Unlike conventional transdermal patches that primarily rely on drug diffusion through the skin, vapour patches combine slow volatilization with limited skin absorption, commonly used for decongestion, sleep aids, or wellness purposes. However, scientific literature specifically validating vapour patches as a distinct drug delivery system is limited, and most information comes from general reviews of transdermal systems. A comprehensive review covering transdermal patch technologies, their types, components, advantages, and limitations, which can serve as a reference for understanding vapour patch concepts within TDDS, is provided by Kumar et al.
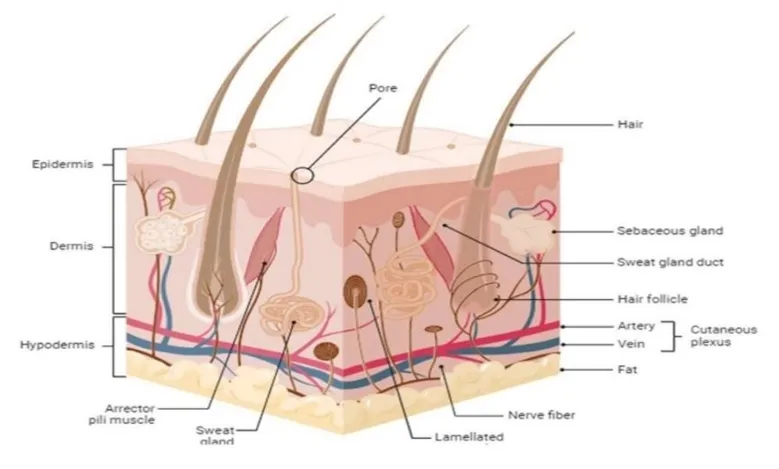
Figure 4 Vapour TDDS Patches
3.4 Reservoir Patches
Transdermal patch with a drug reservoir, aim permeable metallic plastic laminate backing layer, and a porous polymeric membrane that controls drug release over time. Polymeric materials (e.g., hypoallergenic) are used to create the membrane. Fig. 5 shows a Schematic diagram of several transdermal patches. Ethylene vinyl acetate copolymer, genic sticky polymer). The drug is contained in a transdermal patch.
The drug’s molecular dispersion in a polymer matrix, which is part of the preparation, is regulated. Transdermal-Nitro containing nitro glycerine for one-day application, Transdermal Scop carrying scopolamine for three-day application, and Catapres containing clonidine for three-day application are example of commercial transdermal patches with modulated drug release. Application period of seven days.[4]
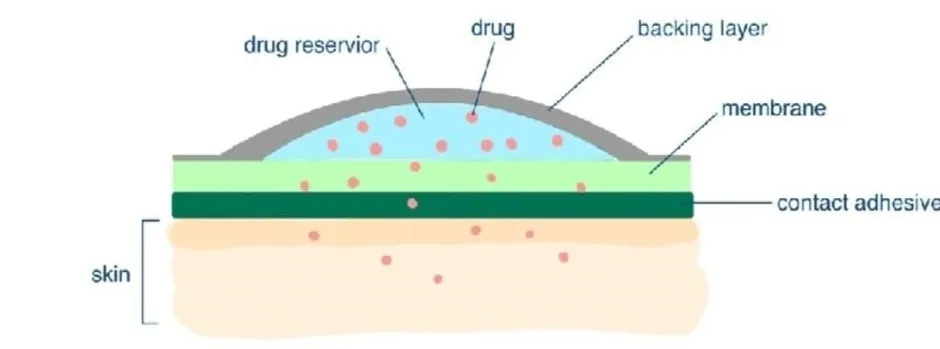
Figure 5 Restorer TDDS Patches
3.5 Micro Reservoir Transdermal Patches [5,6]
Dispersion and a drug reservoir recombined in micro reservoir transdermal patches. The reservoir is made by spreading the drug suspension on a lipophilic polymer after suspending it in an aqueous solution of hydrophilic polymer. A high shear mechanical force is used to [spheres. The drug’s release profile is based on a maintaining a constant drug level in the plasma at a zero-order rate of kinetic drug release. Because the drug dispersion needs to be cross-linked, crosslinking polymeric agents are frequently added stable in terms of thermodynamics.
3.6 Matrix System:[7]
Drug-in-adhesive the drug reservoir is designed to distribute the dug on an adhesive polymer using single layer or multilayer transdermal patches, as shown in Fig.
The sticky polymeric components are melted or solvent cast onto an impermeable backing layer to form a drug-polymer matrix. There are a variety of commercially available products of this type. The NicoDerm patch includes 100 micrograms of oestradiol for a one-day application. The nicotine in the CQ transdermal patch can help you quit smoking for up to 10 weeks.
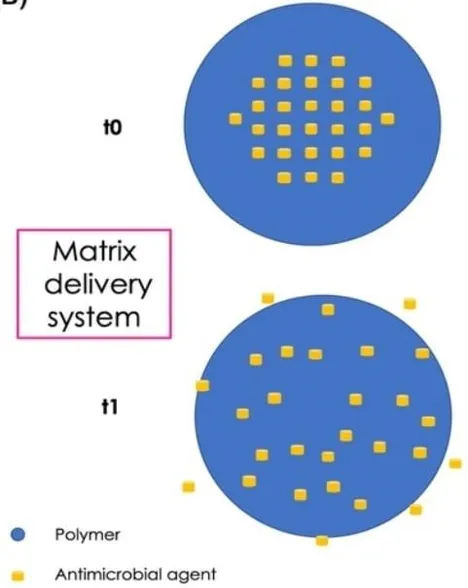
Figure 6 Matrix System
3.7 Matrix Systems: Matrix-dispersion
A hydrophilic or lipophilic polymer matrix serves as the reservoir in a matrix transdermal patch, and the drug is homogeneously disseminated in the matrix. By putting the drug-polymer matrix over a plate with an impermeable laminate backing. Commercially available goods. Nitro-Dur, a matrix dispersion patch containing nitro-glycerine and minitrend, provides a continuous medication flow through undamaged skin The matrix‑type transdermal patch (also called “monolithic” or “drug-in‑adhesive / matrix‑dispersion” system) is one of the most widely used designs for transdermal drug delivery. In this system, the active drug is uniformly dispersed in a semisolid polymeric matrix, which serves as both the drug reservoir and the release-rate controlling layer. This matrix layer is laminated onto an impermeable backing film, and a skin‑adhesive layer (or adhesion rim) ensures the patch remains attached to the skin. Upon application, the drug diffuses from the matrix through the skin barrier into systemic circulation (or locally, depending on the formulation) via passive diffusion controlled by the physicochemical properties of the drug, the polymer, and the skin.
Because of these trade‑offs, matrix‑type patches are generally reserved for drugs and therapeutic situations where the benefits outweigh the constraints — for example, hormones (like estrogenic), pain medications (like certain opioids or NSAIDs), cardiovascular drugs (e.g., nitro-glycerine), and central‑nervous-system agents requiring stable delivery. The matrix design remains the backbone of many modern commercial patches. Moreover, ongoing research explores polymer innovations, skin‑permeation enhancers, and hybrid designs (combining matrix with other permeation technologies) to expand the range of drugs amenable to matrix‑patch [8]
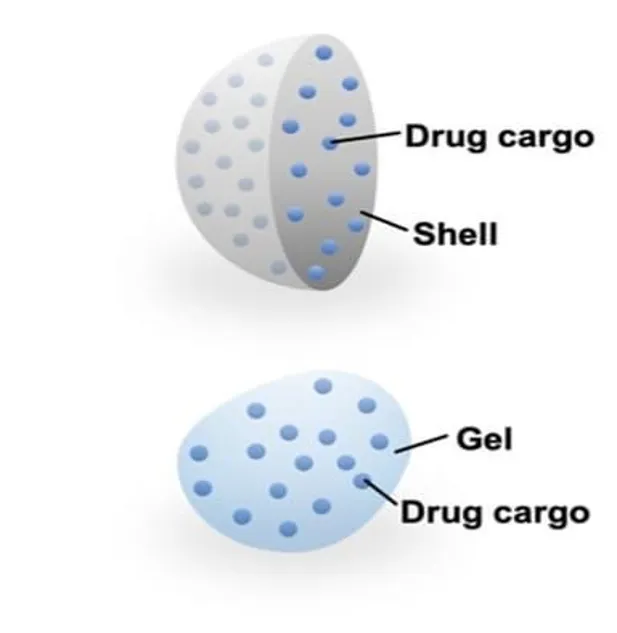
Figure 7 Matrix Dispersion
3.8 Miscellaneous Transdermal Patches
Transdermal patches with adhesive tapes, transdermal gel, transdermal spray, iontophoretic delivery, and phonophoresis delivery are all FDA-approved transdermal matrix delivery techniques, as illustrated in Transdermal patches are used beyond nicotine and opioid analgesia for a wide, “miscellaneous” range of indications where steady systemic or localised delivery improves efficacy, tolerability, or adherence: marketed examples include methylphenidate (DeTrani) for ADHD, rivastigmine for Alzheimer’s disease, retigabine for Parkinson’s disease, nitro-glycerine for angina, scopolamine for motion sickness, combined estrogenic–progestin contraceptive patches, lidocaine and diclofenac patches for local musculoskeletal pain, oxybutynin for overactive bladder, and buprenorphine/fentanyl systems for long-term pain control — each chosen because the skin route provides controlled plasma levels, reduced peakrelated side effects, avoidance of first-pass metabolism and simple, patient-friendly dosing. Several newer and experimental patch formats extend this list: microneedle and dissolvable patches for peptide drugs (including insulin and vaccines), electrically-assisted (iontophoresis) or sonophoresis patches to enhance permeation for otherwise poorly-permeable molecules, smart patches that allow on-demand or sensor-triggered release, and high-loading polymeric matrices or 3D-printed patches designed for large-molecule delivery or multi-drug combinations — all aiming to broaden the therapeutic classes addressable by transdermal delivery. Clinically, the most successful non-analgesic patches (e.g., methylphenidate, rivastigmine, retigabine) show improved adherence or reduced systemic adverse effects compared with oral dosing, while safety considerations are dominated by local skin reactions and the need to avoid overlapping systemic exposure (for example, when combining transdermal and oral forms of the same active). Real-world effectiveness and regulatory acceptance hinge on robust permeation enhancers, adhesive performance, and clear titration/patch-rotation instructions; meanwhile research continues into personalized dosing, higher-load matrices, and delivery of biologics — promising more “miscellaneous” indications (immunization, large-peptide therapies, dermatologic small-molecule combinations) soon. For a comprehensive, up-to-date review that covers marketed patches, emerging technologies (microneedles, smart patches, 3D-printed patches), challenges (skin barrier, adhesion, regulatory issues) and clinical applications across many therapeutic areas, [8]
4. DISEASES TREATED WITH TDDS PATCHES: -
4.1. Osteoarthritis & Musculoskeletal Pain
Musculoskeletal disorders like osteoarthritis, sprains, and rheumatoid arthritis produce inflammation and localized pain. NSAID transdermal patches (diclofenac, ketoprofen, ibuprofen) deliver the drug directly to the affected area, reducing systemic exposure. These patches provide sustained drug release, improve joint mobility, and reduce swelling without causing gastric irritation associated with oral NSAIDs. Their local action results in high drug levels at the painful site with minimal blood concentration. As a result, they are preferred in elderly patients and those with gastrointestinal problems. They are well-tolerated, easy to apply, and useful for long-term pain control.[9]
4.2. Hypertension (High Blood Pressure)
Hypertension requires stable, long-term blood pressure control. Clonidine transdermal patches deliver the drug continuously for 7 days, decreasing sympathetic activity and lowering vascular resistance. Unlike oral clonidine-which may cause peak-dose sedation-transdermal delivery provides smoother pharmacokinetics. The patch improves adherence, especially in elderly patients and those with difficulty swallowing tablets. It also reduces sudden drops in blood pressure and maintains steady therapeutic levels. The controlled delivery mechanism makes it ideal for resistant hypertension or patients who forget multiple daily doses.[10]
4.3. Alzheimer's Disease
Alzheimer's disease involves memory loss and cognitive decline due to reduced acetylcholine levels. The rivastigmine transdermal patch provides continuous delivery of an acetylcholinesterase inhibitor for 24 hours. It maintains stable drug levels and significantly reduces gastrointestinal side effects such as nausea and vomiting compared to oral rivastigmine. The patch improves daily functioning, cognition, and behaviour in mild to moderate Alzheimer's disease. Its ease of use enhances caregiver convenience and patient adherence. It is preferred in elderly patients because of its safety and lower incidence of adverse reactions.[11]
4.4. Depression (Selegiline Transdermal System – EMSAM Patch)
The selegiline transdermal system is used in the management of major depressive disorder (MDD).
Delivered through the skin, selegiline bypasses first-pass metabolism and selectively inhibits monoamine oxidase-B (MAO-B) at lower doses, increasing levels of dopamine, norepinephrine, and serotonin in the brain. This mode of delivery reduces the dietary restrictions normally associated with oral MAO inhibitors. The patch provides continuous 24hour drug release, which helps maintain stable mood and reduces fluctuations linked with oral therapy. Studies have shown that patients tolerant of oral MAOIs often better accept the patch formulation due to fewer systemic side effects and improved convenience.[12]
4.5. Chronic Pain (Buprenorphine Transdermal Patch)
The buprenorphine transdermal patch is used for long-term management of chronic pain, including cancer pain, neuropathic pain, and musculoskeletal conditions. It delivers a steady, controlled dose of opioid analgesic over 7 days, improving adherence and minimizing peaktrough fluctuations. Buprenorphine has a strong affinity for opioid receptors, producing effective analgesia with lower abuse potential compared to stronger opioids. The patch reduces gastrointestinal issues, sedation, and other systemic side effects typically seen with oral analgesics. It is especially beneficial for elderly patients and those requiring continuous pain control. Clinical studies consistently support its effectiveness and safety for chronic pain.[13]
4.6. Pain Management Fentanyl Patch
Fentanyl transdermal patches provide powerful pain relief for chronic cancer pain and severe non-cancer pain. They release the drug continuously for 72 hours, offering more stable pain control than oral opioids.
Because fentanyl bypasses the stomach, it is ideal for patients with nausea or difficulty swallowing. Its controlled delivery reduces sudden peaks and dips in pain.[14]
5. ADVANTAGES AND LIMITATIONS OF TDDS PATCHES:
5.1. Advantages [15]
5.2. Limitation [15]
6. PREPARATION PROCUDURE OF TDDS PATCHES [16]: -
Take the polymer (e.g., PVP/HPMC) in a beaker with a small amount of solvent. Mix 2/3rd of the solvent with other polymers (e.g., PVA) and add it to the beaker, stirring initially at a lower rpm and then at a higher speed. Add the plasticizer and mix it thoroughly. Include the drug with continuous agitation and adjust the volume. Cast the resulting film onto a specially designed glass Mold. Dry the films in an oven at 40°C. Carefully remove the dried films using a sharp blade along the edges. Wrap the dried films in butter paper and store them in a closed container, away from light.
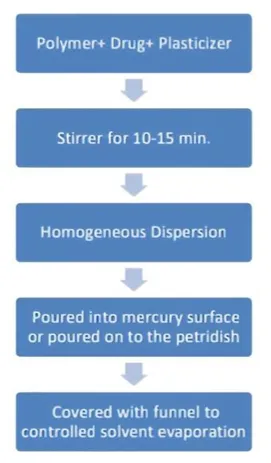
Figure 8 Methods of preparation of Patches
7. CHEMICAL ENHANCERS: -
Chemical enhancers can increase the permeability of the skin by disrupting the lipid structure of the stratum corneum. These enhancers include alcohols, fatty acids, surfactants, and terpenes, which can increase drug penetration by altering the skin’s barrier properties.[17]
7.1 Physical Methods: Techniques such as iontophoresis (the use of an electric current to drive charged molecules through the skin), sonophoresis (ultrasound-assisted drug delivery), and microneedles have been employed to improve drug delivery. Microneedles have gained significant attention due to their ability to create microscopic channels in the skin, allowing for painless and efficient drug delivery.[18]
7.2 Nanocarriers: Nanocarriers such as liposomes, noisome, and solid lipid nanoparticles (SLNs) have been used to enhance the delivery of poorly water-soluble drugs through the skin. These carriers can encapsulate drugs, improving their stability, bioavailability, and penetration ability.
7.3 Microneedle Patches: Microneedles, ranging in length from 25 to 2000 microns, can penetrate the skin's outer layers without reaching the nerves, providing a pain-free method for drug delivery. Microneedle These needles can be made from materials such as silicon, metals, or biodegradable polymers and can be coated with drugs or used to create microchannel for drug diffusion.
7.4 Smart Patches: Smart patches are designed to monitor and respond to physiological changes in real time. For example, insulin patches are designed to release insulin in response to elevated blood glucose levels, providing a personalized approach to diabetes management.
7.5 3D Printing for Patch Fabrication: The application of 3D printing technology allows for the creation of complex, customizable transdermal patches. This technology can be used to create patches with multiple layers for controlled, multi-phase drug release or to incorporate sensors for real-time monitoring of drug delivery. [19]
8. CLINICAL APPLICATIONS OF TDDS PATCHES: -
8.1 Pain Management on TDDS Patches
Transdermal patches are widely used in pain management because they deliver analgesic drugs directly through the skin into the systemic circulation, ensuring steady and prolonged drug levels. These patches avoid first-pass metabolism, reduce dosing frequency, and improve patient compliance, especially in chronic pain conditions. Common drugs used include fentanyl, buprenorphine, lidocaine, and diclofenac, which provide controlled and sustained pain relief for conditions like cancer pain, neuropathic pain, and musculoskeletal disorders. Their noninvasive nature, ease of application, and long duration of action make transdermal patches an efficient alternative to oral or injectable pain medications.[20]
8.2 Hormone Replacement Therapy on TDDS Patches
Transdermal patches for hormone replacement therapy deliver hormones such as estrogenic or a combination of estrogenic and progesterone through the skin into the bloodstream. This method provides steady hormone levels, reduces fluctuations, and lowers the risk of gastrointestinal side effects compared to oral therapy. Transdermal HRT is commonly used to manage menopausal symptoms such as hot flashes, night sweats, mood changes, and vaginal dryness. It also avoids first-pass liver metabolism, making it safer for women with certain risk factors. These patches offer improved compliance due to easy application and controlled release.[21]
8.3 Cardiovascular diseases on TDDS Patches
Transdermal patches are used in cardiovascular therapy to provide controlled and sustained delivery of drugs such as nitro-glycerine, clonidine, and nicotine. Nitro-glycerine patches are commonly used in the management of angina pectoris, where they help dilate blood vessels, improve blood flow, and reduce cardiac workload. These patches maintain steady plasma drug concentrations, minimize dosing fluctuations, and improve patient compliance compared to oral forms. They also bypass first-pass metabolism, leading to effective therapeutic action with fewer systemic side effects. Their ease of use and continuous drug release make them valuable in long-term cardiovascular management.[22]
8.4 Smoking session on TDDS Patch
Transdermal nicotine patches are widely used for smoking cessation as they deliver a controlled amount of nicotine through the skin, reducing withdrawal symptoms and cravings. These patches help maintain stable nicotine levels without the harmful chemicals found in tobacco smoke. They are easy to use, applied once daily, and available in different strengths to support gradual dose reduction. This method improves quit rates, enhances patient compliance, and is often used as part of Nicotine Replacement Therapy (NRT) along with behavioural support. Their steady, non-invasive nicotine delivery makes them effective for long-term smoking cessation.[23]
8.5 Hypertension on TDDS Patched
Transdermal patches are used in hypertension treatment to provide a slow, steady release of antihypertensive drugs such as clonidine. These patches maintain consistent blood pressure control over 24-72 hours, reducing fluctuations seen with oral dosing. They bypass first-pass metabolism, improve patient adherence, and are especially useful for patients who forget daily medications or cannot tolerate oral therapy. Clonidine patches help lower blood pressure by reducing sympathetic activity and providing long-term, non-invasive therapy with fewer systemic side effects.[24]
9. PREPARTION METHOD FOR TDDS PATCHES: -
9.1 Circular Teflon Mold method (Baker and Heller1989):
Solutions containing polymers in various ratios are used in an organic solvent. The calculated amount of the drug is dissolved in half the quantity of the same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. The plasticizer is added to the drug-polymer solution. The total contents are to be stirred for 12 hrs and then poured into a circular Teflon Mold. The Molds are to be placed on a levelled surface and covered with the inverted funnel to control solvent vaporization in a laminar flow hood model with an airspeed of 0.5 m/s. The solvent is allowed to evaporate for 24 h. The dried films are to be stored for another 24 h at 25-0.5°C in a desiccator containing silica gel before evaluation to eliminate aging effects. These types of films are to be evaluated within one week of their preparation have studied bio adhesive film containing ketorolac. Films were cast from organic and aqueous solvents using various bio adhesive polymers namely: sodium carboxymethyl (Na-CMC), hydroxypropyl cellulose (HPC), hydroxypropyl methylcellulose (HPMC), and Carbopol 934. The prepared films were cellulose subjected to investigations for their physical and mechanical properties, swelling behaviours, in-vitro bio adhesion, drug permeation via bovine buccal mucosa, and in-vitro drug release".[25]
9.2 Asymmetric TPX membrane method (Berner and John 1994):
A prototype patch can be fabricated for this a heat-sealable polyester film with a concave of Ime diameter will be used as the backing membrane. Drag sample is dispensed into the concave membrane, covered by a TPX (poly (4-methyl-1-pentene)) asymmetric membrane, and sealed by an adhesive. These are fabricated by using the dry/wet inversion process. TPX is dissolved in a mixture of solvent (cyclohexane) and nonsolvent additives at 60°C to form a polymer solution. The polymer solution is kept at 40°C for 24 hrs and cast a glass plate to a predetermined thickness with a Gardner knife. After that the casting film is evaporated at 50°C for 30 sec, then the glass plate is to be immersed immediately in a coagulation bath. After 10 minutes of immersion, the membrane can be removed, air-dried in a circulation oven at 50°C for 12 h. [26]
9.3 Mercury substrate method:
The drug is dissolved in polymer solution along with plasticizer. It is followed by stirring for 10-15 minutes to produce a homogenous dispersion and poured into a levelled mercury surface, covered with an inverted funnel to control solvent evaporation. Rathore et al have studied that transdermal matrix type patches of terbutaline sulphate were fabricated using ethyl cellulose and cellulose acetate polymer. The transdermal patches of terbutaline sulphate were prepared by solvent casting technique employing a mercury substrate. In the present investigation, various polymeric transdermal patches of terbutaline sulphate were prepared. The effect of permeability enhancers on the permeability of drugs from cellulose acetate and ethyl cellulose patches was studied. The polymeric combinations showed good film-forming properties and the method of casting on mercury substrate was found to give good films".[27]
9.4 IPM membranes method:
The drug is dispersed in a mixture of water and propylene glycol containing carbomer-940 polymers and stirred for 12 h in a magnetic stirrer. The dispersion is to be neutralized and made viscous by the addition of tri-ethanolamine. Buffer can be used to obtain solution gel if the drug solubility in an aqueous solution is very poor. The formed gel will be incorporated in the IPM membrane have studied the drug-in-adhesive transdermal patch and evaluated for the sitespecific delivery of anastrozole. Different adhesive matrixes, permeation enhancers, and amounts of anastrozole were investigated for promoting the passage of anastrozole through the skin of rats in-vitro. The best skin permeation profile was obtained with the formulation containing DUROIPM 8%, and anastrozole 8%. For local tissue disposition studies, the anastrozole 10/16 applied mouse abdominal skin, and blood, skin, and muscle samples were different times after removing the residual adhesive from the skin. High accumulation of the drug in the skin and muscle tissue beneath the patch application site was observed in mice and compared with that after oral administration.[28]
10. EVALUATION TEST FOR TDDS PATCHES [29]: -
10.1. Skin Irritation Test
Evaluates whether the patch causes erythema, itching, redness, or inflammation on human or animal skin. It confirms the biocompatibility of the formulation.
10.2. Surface pH Test
The patch surface pH is measured after slight moistening to ensure it remains compatible with skin pH (4.5-6.5). This avoids irritation and ensures patient comfort.
10.3. Weight Variation Test
Multiple patches are weighed individually. A low percentage variation confirms uniform polymer distribution and consistent patch thickness.
10.4. Thickness Uniformity Test
Thickness is measured at different points using a digital micrometre. Uniform thickness ensures consistent drug release and mechanical stability overtime.
10.5. Flexibility Test
The patch is rolled and unrolled several times to evaluate its mechanical flexibility; good rollability indicates stable polymeric matrix and strong backing membrane.
10.6. Flatness Test
Checks whether the patch surface remains flat without wrinkles or folds during storage. Lack of flatness affects adhesion and drug release.
10.7. Swelling Index Test
Measures how much the patch swells when exposed to moisture or sweat. Controlled swelling ensures the drug release rate remains stable.
10.8. Water Vapour Transmission Rate (WVTR)
Tests how much moisture can pass through the patch. Optimal WWTR is essential to avoid skin maceration and maintain drug stability.
10.9. Tensile Strength Test
Measures the force needed to break the patch. High tensile strength ensures the patch will not tear during application or use.
10.10. Folding Endurance Test
The patch is folded repeatedly until it breaks. Higher folding endurance indicates good elasticity and polymer strength over time.
10.11. Residual Solvent Analysis
Ensures that solvents used during manufacturing are completely removed. High residual solvents can cause toxicity and instability.
10.12. Real-Time Stability Study
Patches are stored at 25°C ± 2°C/60% RH ± 5% for up to 12-24 months to determine accurate shelf-life.
10.13. In-Vitro Permeation Test
Assesses drug permeation across synthetic membrane or animal skin using Franz diffusion cells.
Ensures permeation efficiency does not degrade over time.
11. IMPORTANTS OF EVLUATION TEST: -
What it ensures dose uniformity and consistency- if weight, drug content, thickness vary patch to patch, delivered dose may vary. Confirms adhesion & wearability — good adhesion ensures patch stays on skin for required duration; good pee lability ensures easy removal. Poor adhesion/cohesion can lead to patch detachment or uneven drug delivery.
Verifies drug release and permeation kinetics — release and permeation tests predict how the drug will be delivered through skin over time; important for achieving therapeutic levels. Checks physical stability, formulation integrity, and safety — no crystallization/phase separation, maintained adhesion, stable drug content and release over shelf‑life; no skin irritation. Provides regulatory/quality control assurance — to meet pharmacopeial standards and regulatory requirements for transdermal.[30]
12. RECENT ADVANCES IN THE FIELD OF TDDS PATCHES [31]: -
13.1 Patch technology for protein delivery
13.2 Pain-free diabetic monitoring using transdermal patches
13.3 Testosterone transdermal patch system in young women with spontaneous premature ovarian failure
13.4 Transdermal Patch of Oxybutynin used in overactive bladder (OAB)
13.5 Molecular absorption enhancement technology.
14. CONCLUSION
Transdermal drug rehabilitation patches offer a modern, reliable, and patient-centered approach to supporting addiction treatment and long-term recovery. By delivering medication steadily through the skin, these patches maintain consistent therapeutic levels, which help reduce cravings, prevent withdrawal symptoms, and minimize the chances of misuse. Their noninvasive nature improves patient comfort and compliance, making them particularly suitable for individuals undergoing rehabilitation who may struggle with regular oral dosing. They are especially beneficial for patients who find it difficult to take medicine orally, experience pain during injections, or face issues with swallowing tablets, making patches a more convenient and less stressful alternative. Transdermal systems also avoid first-pass metabolism and reduce gastrointestinal side effects, enhancing their overall safety profile. With continued research and technological advancements, transdermal rehabilitation patches are expected to play an even more significant role in de-addiction programs by providing safer, more controlled, and more convenient drug delivery options.
REFERENCES



Shreyash Bawage, Dr. Ganesh Tolsarwad, Mahesh Mukta, A Review on Transdermal Drug Delivery Patches, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 810-825. https://doi.org/10.5281/zenodo.21164352
 10.5281/zenodo.21164352
10.5281/zenodo.21164352