
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,4,5 Shri Gurudatta Shikshan Prasarak Sanstha Institute of Pharmacy, Kaulkhed, Akola
6 PRMMS Anuradha College of Pharmacy Chikhli
One of the features of solid tumors includes hypoxia, which leads to therapeutic resistance, metastasis, and poor prognosis. The conventional approaches used to detect and target hypoxia often lack the accuracy needed for the clinical translation. Advances in nanomedicine have enabled oxygen-responsive nanoparticles which can release the drug within hypoxic tumor microenvironments, but the efficacy further depends on the accurate hypoxia characterization. AI now provides various tools to overcome this barrier. By analyzing the MRI, PET, and multimodal imaging data, AI models can generate voxel-level hypoxia maps, guiding the design of nanoparticles with optimized drug loading and release kinetics. In addition, AI also helps in the incorporation of hypoxia biology, including HIF-mediated signaling and metabolic reprogramming, with the predictive modeling to ensure the personalization of treatment. Various emerging strategies include hypoxia-activated prodrugs, biomimetic nanocarriers, and dual-function systems that combine the therapy with real-time monitoring. In spite of these advances, challenges remain, such as model interpretability, clinical validation, manufacturing scalability, and regulatory acceptance. Looking forward, the combination of AI, quantum computing, and nanotechnology has the potency for the accurate, patient-specific therapies with respect to the tumor physiology. This review highlights current progress at the intersection of tumor hypoxia biology, AI-guided imaging, and oxygen-responsive nanomedicine, also highlighting the future aspects and challenges in incorporating these innovations into precision oncology.
An insufficient oxygen delivery to particular areas or organs, above and beyond their normal demand within the tissue microenvironment, is known as hypoxia, which is a substantial physiological stress. This behavior is especially common in solid tumors and other malignant tissues. A feature of many solid tumors is hypoxia, which is brought on by an imbalance in the supply and consumption of oxygen (O2) by rapidly multiplying tumor cells. Normal tissues may be disrupted by the increased production of reactive oxygen species (ROS) caused by the hypoxic TME. Additionally, it causes treatment resistance and interferes with cell cycle regulation, which increases the risk of cancer recurrence. The effectiveness of immunotherapy, chemotherapy, and radiation therapy is diminished by hypoxia. Over the past ten years, there has been a lot of interest in gene therapy, medication administration, and cancer imaging due to the unique physicochemical characteristics and biological consequences of different nanoparticles that target hypoxia. Thanks to the development of nanotechnology, nanomaterials have recently provided novel insights into the treatment of tumor hypoxia. These nanomaterials can aid in the treatment of tumor hypoxia in a number of ways, such as by generating or transporting oxygen in a targeted manner or by creating nanostructures changed by hypoxia-activated chemical bonds. By carefully targeting TME characteristics like hypoxia and acidosis, nanoparticles can enable more accurate drug delivery at the target location. [1], [2]
The scientific world has taken notice of a number of nanotechnology-based tactics, including tissue reoxygenation, HIF-1 activity suppression, genetic silencing of HIF-1 expression, and drug encapsulation that interferes with the HIF-1 signaling pathway. [3]
Using membrane-coated nanoparticles for camouflage is another creative way to enhance the delivery of anticancer medications to hypoxic tumors. Red blood cell-coated poly (lactic-co-glycolic acid) nanoparticles (RBC-PLGA-NPs) carrying the anticancer drug curcumin and the hypoxia-activated chemical tirapazamine were made for a study.
This mixture successfully triggered caspases, produced reactive oxygen species (ROS), and harmed the DNA of malignant cells. [4]
However, reliable mapping and assessment of tumor hypoxia require successful deployment, which is often not possible with routine imaging or biopsy procedures at sufficient resolution or reproducibility. AI currently offers a means of closing this gap. It was demonstrated that it was possible to predict hypoxia for HN tumors voxel-wise from a 2D deep learning network using FDG-PET scans as inputs. There was a good correlation between the hypoxic volume forecasts in test cases and FMISO-PET (Pearson R = 0.96; p < 0.001). [5]
Pathophysiology and Implications of Tumor Hypoxia
A common characteristic of solid tumors is hypoxia, which arises when the tumor grows too quickly to meet the oxygen supply and when aberrant blood arteries supplying the tumor form, impairing blood flow. A characteristic of enhanced malignant progression and decreased response to treatment is tumor hypoxia. The efficiency of curative treatment is negatively impacted by poorly oxygenated tumors, according to a substantial body of clinical and experimental evidence. [6]
Tumor hypoxia that promotes cancer cell survival will:
1) result in resistance to chemotherapy and chemo radiation; and
2) raise the likelihood of metastases, which could hasten patient death.
3) Rapid tumor cell proliferation, aberrant tumor vasculature, high interstitial pressure, or inadequate oxygen delivery can all cause tumor growth, invasion, and resistance to treatment. Hypoxia regulates these processes. Together, these characteristics may increase a tumor's capacity to spread.Within solid tumors, hypoxia can be characterized as either acute, chronic, or cyclical. Cycling hypoxia is characterized by tumors that are periodically exposed to hypoxia and then reoxygenated; this is linked to the enhancement of typical cancer markers. This contributes significantly to the development of resistance to chemotherapy and radiation therapy.[7],[8]
Hypoxia-Mediated Pathway Intervention and Cancer Treatment
The pathobiology of tumor growth is significantly impacted by hypoxia, which also affects several cellular functions that are essential to the development of cancer. Among these impacts are changes in cell division, tumor tissue survival in unfavorable conditions, the capacity to cross migration barriers, immune system surveillance evasion, and diffusion to other organs. Thus, focusing on hypoxia-mediated pathways has become a viable cancer treatment approach. The key mediator causing hypoxic responses is hypoxia-inducible factor-1 (HIF), which is made up of heterodimeric factors that are further divided into HIF-1, HIF-2, and HIF-3. Prolyl hydroxylases (PHDs) hydroxylate proline residues on the α-subunit of HIF-1 under normoxic conditions, resulting in ubiquitination and subsequent destruction through the 26S-dependent proteasome and the von Hippel–Lindau protein (pVHL).HIF-1α, on the other hand, stabilizes and phosphorylates PHD by inhibiting its activity in hypoxic conditions. After that, HIF-1α binds to hypoxia-responsive proteins and dimers with HIF-1β. elements (HREs), and alters how target genes are expressed. HIF-1α is involved in a number of cellular functions and shares similarities with HIF-2α and HIF-3α. During embryonic development, HIF-2α, which is primarily expressed in adult vascular endothelial cells, the heart, lungs, and placenta, is essential for controlling the expression of genes that affect angiogenesis and metabolic tolerance, including vascular endothelial growth factor (VEGF), glucose transport proteins (GLUT-1 and GLUT-3), and erythropoietin (EPO). Additionally, HIF-2α promotes tumor growth via the macrophage lactate/HIF-2α/ATP6vod2 cascade and upregulates the transcriptional activity and expression of HIF-3α. Numerous carcinogenic processes, such as nutritional deprivation, angiogenesis, metabolic alterations, acidosis, and immunosuppression, are encouraged by the adaptive response to oxygen mediated by HIF-1. Twist-related protein, or TWIST, is expressed when HIFs are present.
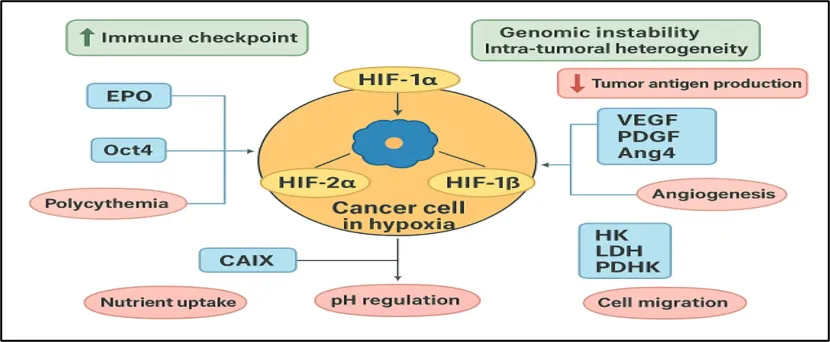
Fig.1 Hypoxia-Inducible Factors (HIFs) and their role in Cancer under Hypoxia
Hypoxia (low oxygen levels) in tumors promotes cancer progression, metastasis, and resistance to anticancer drugs. Targeting HIF-1α is a key therapeutic strategy through gene silencing or inhibition of the PI3K/Akt/mTOR pathway. Inhibition of HSP90, which regulates HIF-1α, has shown potential in cancer treatment. Hypoxia also increases the expression of VEGF, CA IX, GLUT-1, GLUT-3, and CD73, promoting tumor growth and survival. Other approaches include reducing cellular oxygen consumption, targeting tumor metabolism, and using VEGF-based therapies to improve blood vessel formation. Since hypoxia causes metabolic reprogramming that helps tumor cells survive stress, targeting these metabolic changes is a promising anticancer strategy.Targeting hypoxic cancers may benefit from reversing the adaptation of hypoxia-induced cell death signals. Protease inhibitors, protein kinase inhibitors, cytotoxic agents, and other natural and synthetic drugs that target early or late pathways are presently being studied and shown to be effective in sensitizing cancer cells. [10],[11],[12]
Current approaches to hypoxia detection
Tumor oxygen partial pressure (pO₂) was assessed in 86 patients with primary cervical carcinoma using an Eppendorf pO₂ histograph and immunohistochemically detection of pimonidazole binding. Patients received a single intravenous injection of pimonidazole (0.5 g/m²), and 10–24 hours later, pO₂ measurements and tumor biopsies were obtained. Tumor oxygenation was quantified as the median pO₂ and as the proportion of values at or below 10 mmHg (HP10), 5 mmHg (HP5), and 2.5 mmHg (HP2.5). Hypoxia was further evaluated by immunohistochemistry using monoclonal antibodies against reductively activated pimonidazole. Binding intensity was scored microscopically, with each tumor characterized by both the maximum pimonidazole staining score and the cumulative area of staining across scores 1 to 4.
Measurement of pO2 distribution and bioreductive enzymes in human malignant brain tumors in the below fig.2[13]
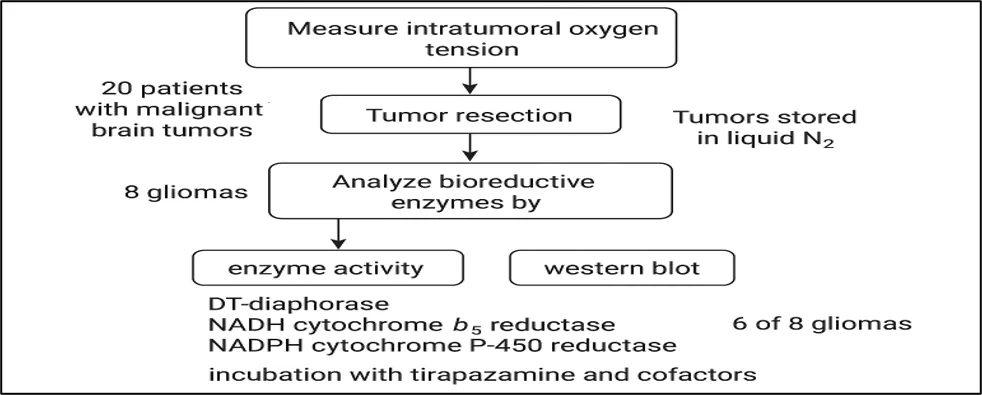
Fig.2 Incubation with Tirapazamine and cofactors
Hypoxia marker labeling in tumor biopsies
The CCI-103F hypoxia marker was assessed in dogs with solid tumors that arise normally. Two biopsies were taken from each of the seven tumors, for a total of 14 samples. To determine the most accurate estimate of the CCI-103F-labeled region throughout the entire sample, four to six consecutive slides from every 100–150 μm interval were evaluated after each biopsy was serially sectioned. One, two, or four slides were randomly selected from each biopsy in order to investigate the impact of reduced sampling. The labeled area obtained from these subgroups was then compared with the full-slide estimate. The random selection procedure was carried out a thousand times for every biopsy.[14]
Nano particle drug delivery
The initial size of nanoparticles, especially during enzyme-induced size reduction, is a critical factor in determining how responsive they are to particular stimuli. However, aberrant vascular permeability and compromised lymphatic drainage combine to produce a dense extracellular matrix and increased interstitial fluid pressure (IFP) in tumors. These factors reduce the effectiveness of size-reducible systems for drug Despite their intricate structure and function, nanoparticles are currently being modified to take advantage of characteristics of the tumor microenvironment, including tissue density, hypoxia, acidity, and aberrant protein expression. Techniques include size enlargement to improve tumor retention, enzyme-mediated breakdown to enable deeper penetration, and acid-sensitive connections for regulated drug release. Chemotherapy based on nanocarriers has been investigated extensively in an effort to increase medication absorption while reducing harm to healthy tissues.¹ Nevertheless, a number of nanoscale delivery methods continue to face issues that jeopardize therapeutic results, such as inadequate loading stability and early drug release.² Stimuli-responsive nanomedicines, which allow for controlled, on-demand medication delivery, have been created to solve these problems.[9]Reducing hypoxia can greatly increase the efficacy of next therapies. Using a nanobioreactor made of dextran sulfate-modified catalase, which reacts with the increased hydrogen peroxide in the tumor microenvironment to produce oxygen, we provide a dual oxygen delivery approach in this work. A secondary oxygen supply is created concurrently by the slow release of oxygen that has been preloaded into the nanoparticles. In PANC-1 pancreatic cancer cells, this dual platform showed continuous oxygen release for over six hours. [15],[16],[17]
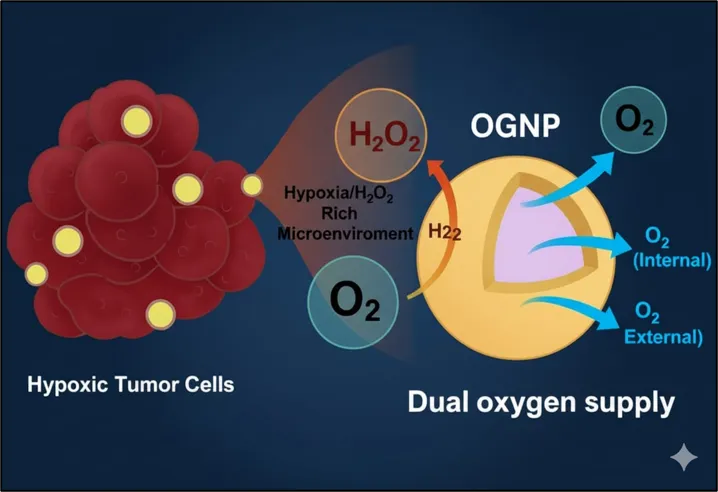
Fig.3 Dual Oxygen Supply to Hypoxic Tumor Cells via OGNP
AI in prediction & Mapping Tumor Hypoxia
MRI
An overview of recent research on applying artificial intelligence to predict survival in patients with brain tumors using MRI is given in this paper. In this field, both machine learning and deep learning methodologies show a great deal of potential. Although no single approach can be regarded as universally ideal because performance is influenced by several variables, comparative evaluations of various models showed great performance across studies for both overall survival (OS) and survival classification (SC). Importantly, features from diffusion-based methods (DWI/DTI) and perfusion-weighted imaging (PWI) consistently showed value for both prediction tasks. The usefulness and dependability of AI-driven prognostic models are further improved by the incorporation of quantitative imaging, which is becoming more standardized and reproducible across imaging systems. [18]
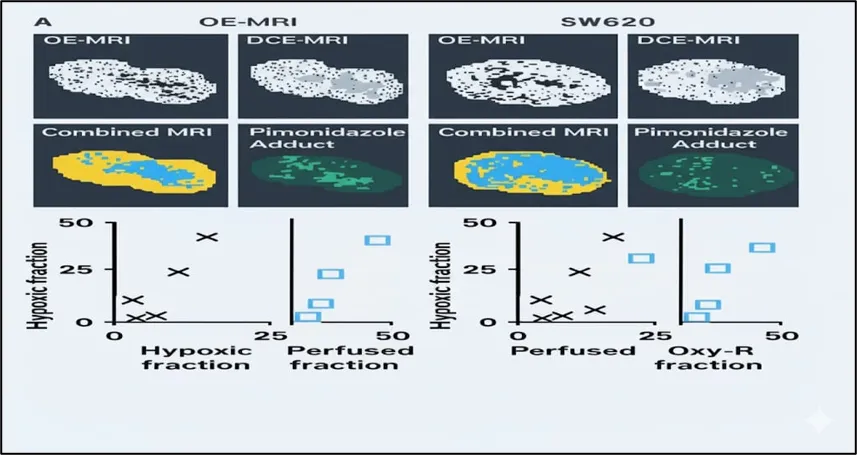
Fig.4 Magnetic Resonance Imaging (MRI) maps and corresponding scatter plots for tumor analysis
A metric for measuring the hypoxic fraction in several tumor models is the perfused Oxy-R fraction. To differentiate between enhancing and nonenhancing voxels, representative OE-MRI and DCE-MRI maps from 786-0-R (A) and SW620 (B) tumors were binarized. Voxels in the integrated MRI datasets were categorized as nonperfused (gray), perfused Oxy-E (yellow), or perfused Oxy-R (blue). Using immunofluorescence mapping of pimonidazole adduct formation, tumor hypoxia was further assessed. The Oxy-R fraction and the hypoxic fraction in 786-0-R tumors showed a substantial connection, which remained when the study was restricted to perfused voxels. The Oxy-R fraction and the hypoxic fraction in 786-0-R tumors showed a substantial connection, which remained when the study was restricted to perfused voxels. On the other hand, MRI tended to overstate the hypoxic fraction in SW620 tumors, while the Oxy-R fraction did not significantly correlate with it. Interestingly, a strong association was found when the study was limited to perfused Oxy-R voxels (blue squares). The optical probe [Ru(dpp)₃] Cl₂ was used to monitor the intracellular oxygen levels [19].
Pet Paper Study
Short Note
This study evaluated a pharmacokinetic compartmental model for measuring tumor hypoxia using dynamic PET imaging and the hypoxia-specific tracer 18F-fluoromisonidazole (FMISO). The model included three intratumoral compartments—normoxic, hypoxic, and necrotic tissues—within a normal tissue background. An arterial input function was used to generate time-activity curves for each voxel based on kinetic parameters obtained from FMISO-PET scans of head and neck cancer patients. The results showed that compartmental kinetic modeling can reliably quantify tumor hypoxia, although its accuracy depends on the shape of the input function and the analysis method used. This work provides valuable guidance for improving and designing clinical dynamic FMISO-PET studies for accurate assessment of tumor hypoxia.[20]
Prediction using decision fusion
There is potential for preventing negative consequences if a dynamic system is able to continuously monitor and detect changes in physiological condition linked to the beginning of hypoxia. We introduce a parallel M-ary decision fusion architecture-based real-time hypoxia monitoring system. The system generates estimations of the degree of hypoxia as outputs and uses altitude data and blood oxygen saturation readings as inputs. Novel temporal evolution models are developed to explain the dynamics of blood oxygen saturation and functional impairment under various altitudinal situations in order to bolster this framework. These models make it easier to precisely track various hypoxia conditions in relation to the length of time an individual is exposed to altitude. The system combines data to produce global estimates of hypoxia severity using a Bayesian decision-making technique. The accuracy and resilience of the suggested detection methods are demonstrated through validation on both artificial and real-world datasets. [22]
AI-guided design & optimization O2 responsive nanoparticles
Short Note: Hypoxia-Responsive Nanotherapeutics
Hypoxic tumor microenvironments provide an opportunity for tumor-specific drug delivery. Nanomedicines can be designed to target hypoxia-induced changes in the tumor microenvironment (TME). Researchers are developing stimuli-responsive nanoparticles that release anticancer drugs in response to acidic pH, low oxygen levels, and intracellular redox conditions present in tumors. Additionally, hypoxia-sensitive prodrugs and nanocarrier systems enable controlled and targeted drug release at the tumor site, improving treatment effectiveness while reducing damage to healthy tissues.[23]. Hypoxia-responsive systems increase the effectiveness of radiation and chemotherapy by activating in low oxygen environments. [24] One characteristic of solid tumors is hypoxia. Most healthy tissues with a plentiful blood supply have an oxygen tension of between 30 and 70 mmHg. The oxygen tension surrounding the majority of tumor cells, on the other hand, ranges from 2.5 mmHg to 7.5 mmHg.[25] Hyperoxic areas can hasten the development of the tumor barrier and boost cytokine secretion.[26] These aberrant tissue conditions confer tumor cells distinct physical, chemical, and biological properties, including high redox potential and low pH Researchers can enhance the creation of novel nanomaterials and provide more efficient diagnostics and treatment by having a better understanding of their properties. [27]
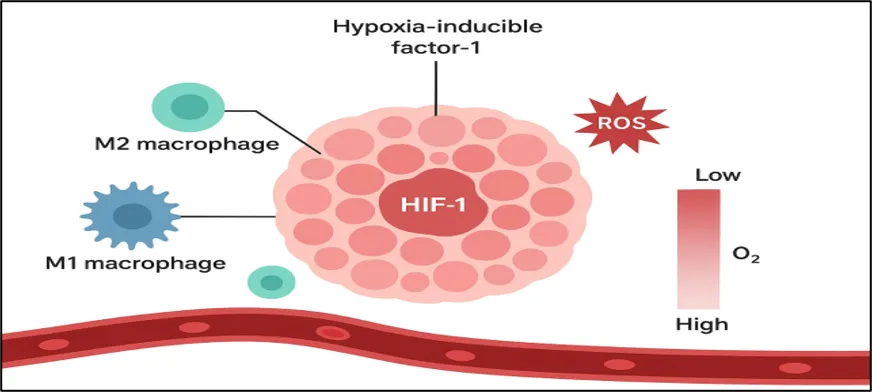
Fig. 5 Hypoxia-Inducible Factor 1 (HIF-1) and Macrophage Polarization in the Tumor Microenvironment.
In order to treat hypoxic malignancies, we engineered a supramolecular albumin nanoparticle (SHC4H) modified by AC4A. SHC4H is made via the self-assembly of reduced HSA chains modified by AC4A (HSA-AC4A), the mitophagy inhibitor (HCQ), and the mitochondrial-targeting Type I photosensitizer (SMNB), as shown in Fig. 1a. The guest molecules (HCQ and SMNB) are released when the host molecule (AC4A) on SHC4H is reduced to aminocalixarene (NH2C4A), which has a low drug affinity, under hypoxia. By alkalinizing lysosomes, interfering with pro-survival metabolic adjustments, and elevating oxidative stress in tumor cells, HCQ prevents hypoxia-induced mitophagy. Additionally, the liberated SMNB regains its initial fluorescence, allowing for real-time treatment process monitoring. [28]
SMNB then damages mitochondria and intensifies oxidative stress by producing ROS via the electron transfer pathway when exposed to 660 nm light. In addition, autophagic flux blockade causes the tumor cells to undergo a dual attack of ROS-induced mitophagy and lysosomal destruction, which results in mitophagy stress, autophagosome accumulation, oxidative stress amplification, and ultimately cell death (Fig. 1b). We further investigate the efficacy of this approach across various cell types because there aren't many studies on mitophagy-related therapy in the treatment of hypoxic tumors. According to our findings, SHC4H+hv therapy exhibits superior therapeutic effects via several cell death pathways in hypoxic tumors that are B16, 4T1, PANC1 (expressing caspase-3), and MCF-7 (deficient in caspase-3). In conclusion, SHC4H effectively treats hypoxic tumors by coordinating mitophagy regulation and mitochondrial disruption to cascade-amplify oxidative stress.[29]
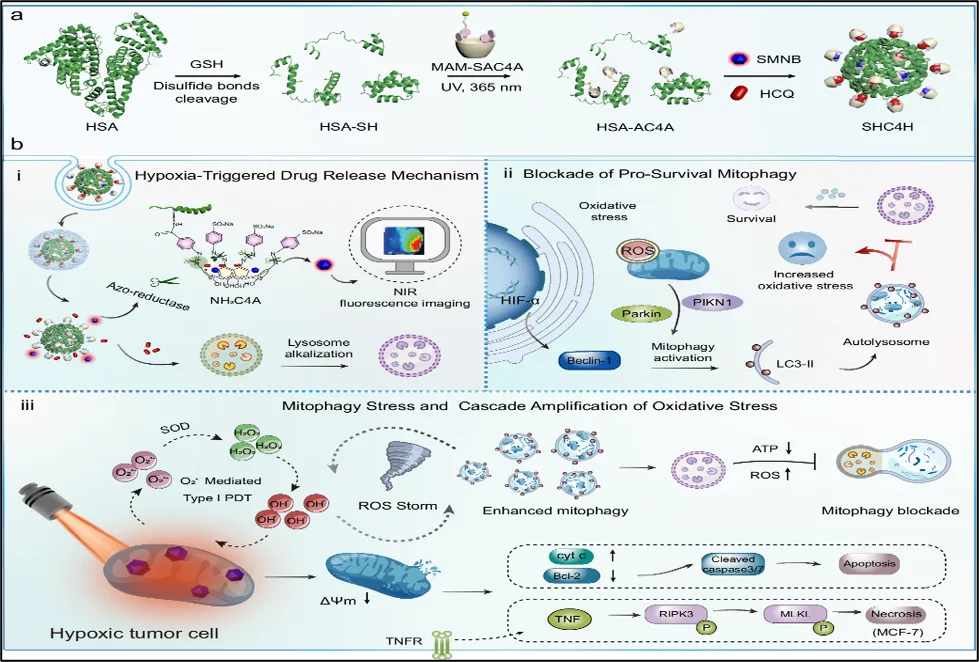
Fig.6 Schematic illustration of the preparation procedure of SHC4H and the anti-tumor mechanism under hypoxia. (6)
A photoclick chemical procedure is used to conjugate HSA with free thiol groups to methacrylamide-monomodification sulfonate modified azocalixarene (MAM-SAC4A). Following the encapsulation of SMNB and HCQ, SHC4H was created by a self-assembly method. b i-ii. SHC4H's fluorescence imaging and hypoxia-responsive drug release capabilities. In order to prevent hypoxia-induced pro-survival mitophagy, HCQ alkalized lysosomes prior to laser irradiation, which led to an imbalance and elevated oxidative stress. Laser irradiation caused O2•--mediated type I M-PDT in SMNB, and the ongoing buildup of mitophagy flux exacerbated oxidative stress and created an intracellular ROS storm. separate tumor cells died in two separate ways as a result of the ROS storm inside the mitochondria. [30]
Useful in personalized therapy
AI-guided tumor hypoxia prediction enhances nanoparticle design and allows for tailored treatment. [31] AI algorithms may evaluate patient-specific hypoxia maps using MRI or PET imaging to determine the extent and geographic distribution of oxygen deprivation within malignancies [32]. By modifying the surface, modifying the medication loading, or altering the release kinetics, oxygen-responsive nanoparticles can be customized for every patient. Nanoparticles like SHC4H, for instance, show distinct treatment pathways in cancers that express caspase-3 (apoptosis-dominant) and those that lack it (necroptosis-dominant), underscoring the need for pathway-specific customization. Additionally, hypoxia-responsive photosensitizers' inherent fluorescence recovery enables real-time therapy response monitoring, which AI may interpret to dynamically modify treatment parameters like dosage and irradiation duration (9). Thus, AI-assisted oxygen-responsive nanomedicines hold great potential for truly personalized cancer therapy [33]
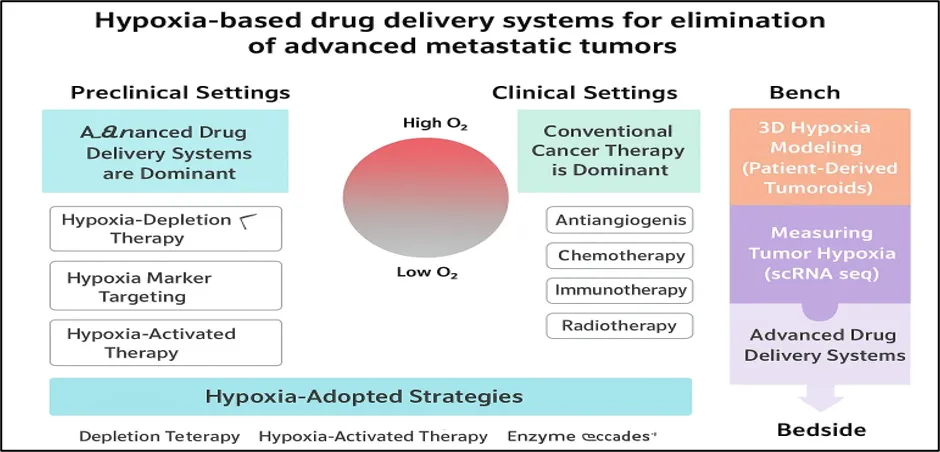
Fig.7 Hypoxia-based drug delivery systems for elimination of advanced metastatic tumors
CHALLENGES
Pulse sequence parameters, GBCA injection procedures, and post-processing methods are only a few of the numerous causes of variability in perfusion MRI that impact the accuracy of hypoxia-related biomarkers like rCBV. [34] A fundamental tenet of DSC modeling is broken by contrast leakage in higher-grade gliomas, which results in imprecise CBV estimation and a misinterpretation of tumor growth in relation to treatment-related effects. [35]
The difference between normalization and standardization of rCBV is crucial because standardized methods improve cross-site repeatability by lowering variability specific to patients and protocols.[36] Although ASL and DCE methods have more complicated modeling requirements and lower signal-to-noise ratios than DSC, they can nevertheless offer supplementary data on perfusion and oxygenation dynamics.[37] Since AI models rely on the prediction of hypoxic regions to maximize oxygen-responsive nanoparticle medication delivery, accurate imaging biomarkers are crucial since errors in CBV or CBF estimate directly impair this prediction [38].Hypoxia in tumors decreases the efficacy of many treatments, changes the tumor microenvironment by attracting pro-tumor immune cells, inhibits drug delivery because of aberrant vasculature, and causes drug resistance through HIF-1-related pathways. These elements make it difficult for AI models to identify hypoxic areas with accuracy and to optimize the drug administration of oxygen-responsive nanoparticles [39]
FUTURE ASPECTS
AI is crucial for improving the formulation and administration of treatments based on nanoparticles. Researchers can improve targeting capabilities, anticipate how nanoparticles will interact with biological systems, and minimize any adverse effects by using machine learning algorithms. By more effectively identifying potential chemicals and formulations than conventional techniques, AI-driven models can hasten the creation of innovative nanomedicine. By maximizing the delivery of nanomedicine to attain and sustain the ideal medication concentration in the bloodstream and targeted regions, artificial intelligence (AI) and related technologies have the potential to completely transform the treatment of cancer.[40] In the future, complex biological ecosystems can be rapidly stimulated thanks to AI and quantum computing. This speeds up the creation of next-generation nanomedicines and improves nanoparticle modeling. Since people typically lack the capacity to objectively evaluate the diagnosis and treatment decisions made by doctors, artificial intelligence (AI) in healthcare has special qualities when compared to other domains, such as the unique trust relationship between doctors and patients.[41] This dynamic emphasizes the necessity for AI systems to be transparent, ethnically sound, and therapeutically safe in addition to being technically good. In contrast to medical equipment, There are currently no widely recognized methods for ensuring the quality of AI. Future artificial intelligence (AI) will therefore be a risk-informed framework that suggests evaluating particular risks and problems early in the process and then putting in place customized strategies to lower these risks. Transparent and morally sound AI systems may become possible in the future [42]
CONCLUSION
Tumor hypoxia is a major obstacle in cancer treatment because it promotes drug resistance, immune evasion, and poor therapeutic outcomes. Nanomedicine provides promising solutions through hypoxia-responsive and stimuli-activated nanoparticles that enable targeted drug delivery. Artificial Intelligence (AI) further enhances these approaches by accurately identifying hypoxic regions, optimizing nanoparticle design, and supporting personalized treatment strategies with real-time monitoring. Despite significant progress, challenges such as the limited interpretability of AI models, variability in imaging methods, manufacturing difficulties, and regulatory concerns remain. Future developments in explainable AI, multifunctional nanocarriers, scalable production techniques, and advanced computational technologies are expected to improve clinical translation. The integration of AI, hypoxia biology, and nanomedicine represents a promising pathway toward precision cancer therapy and better patient outcomes.
REFERENCES

Urmila Tiwaskar, Purva Gupta, Pranali Asolkar, Gayatri Jawanjal, Huda Tazeen Anees Shah, Jogeshwari Burungale, AI-Guided Prediction of Tumor Hypoxia for Oxygen-Responsive Nanoparticle Drug Release, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 119-133. https://doi.org/10.5281/zenodo.20484165
 10.5281/zenodo.20484165
10.5281/zenodo.20484165