
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Student Bhujbal Knowledge City Met’s Institute of Pharmacy Adgaon, Nashik-422003 2024-2025
5Assitant professor Bhujbal Knowledge City Met’s Institute of Pharmacy Adgaon, Nashik-422003 2024-2025
Background:Antibiotic resistance is a growing global concern, particularly in healthcare settings. The pattern of antibiotic use and resistance varies across age groups and is further influenced by the presence of comorbid conditions. Understanding these patterns is crucial for optimizing antibiotic stewardship and improving patient outcomes. Objectives:To evaluate and compare the usage patterns and resistance profiles of antibiotics in paediatric and adult patients, with and without comorbidities, admitted to a tertiary care hospital.Methods:This prospective observational study was conducted over a defined period in a tertiary care hospital. Patients were categorized into paediatric and adult groups, and further stratified based on the presence or absence of comorbidities. Data were collected on patient demographics, diagnosis, prescribed antibiotics (including dosage, route, and duration), and culture sensitivity reports. The organisms isolated and their resistance patterns were also analyzed. Results:Preliminary findings indicate a higher frequency of broad-spectrum antibiotic usage in adult patients with comorbidities compared to other groups. Resistance patterns showed notable differences, with a higher prevalence of resistant organisms in patients with underlying health conditions. Culture sensitivity testing was not uniformly performed across all cases, highlighting a gap in current clinical practice.Conclusion: Antibiotic usage and resistance patterns vary significantly between paediatric and adult populations, especially in the presence of comorbidities. These findings underscore the need for age- and condition- specific antibiotic stewardship protocols to combat resistance effectively and ensure rational drug use.
The discovery of antibiotics marked one of the most transformative moments in medical history, redefining the landscape of infectious disease treatment and dramatically increasing life expectancy worldwide. These bioactive compounds, initially derived from natural sources such as fungi and soil-dwelling microorganisms, are characterized by their ability to selectively inhibit or kill bacteria without causing significant harm to the host organism. Since the accidental discovery of penicillin by Alexander Fleming in 1928, the "antibiotic era" has ushered in successive generations of increasingly sophisticated agents that target a broad range of bacterial pathogens.
Antibiotics exert their effects through diverse mechanisms, including disruption of cell wall synthesis, inhibition of protein or nucleic acid biosynthesis, and interference with essential metabolic pathways. Their classification reflects both their structural diversity and spectrum of activity, ranging from narrow-spectrum agents that target specific bacterial groups to broad-spectrum antibiotics with wide-reaching effects. However, the very success of antibiotics has paradoxically contributed to their greatest threat: antimicrobial resistance (AMR). Misuse, overprescription, and extensive agricultural application have accelerated the emergence of resistant strains, challenged the efficacy of once-reliable therapies and threatened to return humanity to a pre-antibiotic era.
In recent years, the field of antibiotic research has undergone a paradigm shift in response to this global crisis. Traditional drug discovery pipelines, which have stagnated for decades, are now being reimagined through the lens of technological convergence and ecological innovation. Several notable trends characterize this contemporary phase of antibiotic science:
These evolving trends signify a departure from traditional approaches and emphasize a more interdisciplinary, data-driven, and ecologically conscious framework for antibiotic innovation. As the global health community confronts the twin challenges of resistance and discovery fatigue, this thesis seeks to critically explore the scientific, clinical, and technological frontiers of antibiotic research—situating current developments within their historical context and evaluating future directions for sustainable antimicrobial therapy.
Antibiotic resistance is a growing global concern, particularly in healthcare settings where infections are prevalent. The comparative assessment of antibiotic use and resistance in paediatric and adult patients with and without comorbidities in a tertiary care hospital is crucial for understanding prescribing patterns, resistance trends, and the impact of underlying health conditions on treatment outcomes.
Background
Antibiotics have revolutionized modern medicine, significantly reducing morbidity and mortality associated with bacterial infections. However, inappropriate use and overuse have led to the emergence of resistant bacterial strains, complicating treatment strategies. Paediatric and adult patients exhibit distinct physiological responses to antibiotics, and the presence of comorbidities further influences drug efficacy and resistance development.
Rationale for the Study
The study is motivated by the need to optimize antibiotic prescribing practices and reduce the incidence of resistant infections. Special attention is given to how comorbid conditions influence both the prescription patterns and the development of antibiotic resistance. Through a comprehensive prospective observational study, valuable insights will be generated to inform clinical guidelines and improve patient outcomes.
Further background and detailed discussion of the global impact of antibiotic resistance is provided here, highlighting previous research and current challenges in antibiotic management.
In tertiary care hospitals, antibiotics play a critical role in managing infections, particularly among paediatric and adult patients with and without comorbidities. Various classes of antibiotics are commonly prescribed, including cephalosporins, carbapenems, fluoroquinolones, penicillin, macrolides, aminoglycosides, and glycopeptides, each with distinct mechanisms targeting bacterial pathogens. However, the increasing misuse and overprescription of these drugs contribute significantly to antimicrobial resistance (AMR), making infections harder to treat and leading to prolonged hospital stays and higher healthcare costs. Studies indicate that antibiotic consumption in tertiary care settings often exceeds recommended levels, with the frequent use of broad-spectrum antibiotics exacerbating resistance issues. A major challenge in antibiotic stewardship is the lack of adherence to established prescribing guidelines, such as WHO’s Aware classification, which categorizes antibiotics based on safety and necessity. The emergence of multidrug-resistant bacteria further complicates treatment protocols, necessitating stricter monitoring and targeted interventions to ensure optimal antibiotic use. Implementing antimicrobial stewardship programs and promoting rational prescribing practices are crucial steps in mitigating resistance and improving patient outcomes. This study aims to provide a comparative assessment of antibiotic usage and resistance patterns among different patient groups, offering valuable insights into the evolving trends in antibiotic efficacy and the need for enhanced stewardship measures.
NEED FOR STUDY :
AIM AND OBJECTIVE:
AIM:
To compare the dynamics of antibiotics utilization & resistance trends across pediatric & adult populations – in a tertiary care hospital.
OBJECTIVES:
METHODOLOGY AND MATERIALS:
Study Design:
This study was designed as a prospective observational study conducted over a period of six months in a tertiary care hospital. The objective was to systematically collect and analyze data from a diverse patient population to understand diagnostic and treatment patterns. The observational nature of the study ensured that the clinical outcomes were assessed without any intervention or alteration in the standard treatment protocols. A total of 500 patients were included in the study, categorized into two distinct age groups for comparative analysis: pediatric patients (0–18 years) and adult patients (19 years and above).
Study Setting:
The study was conducted in a tertiary care hospital equipped with a wide range of specialized medical departments. The hospital is recognized for its advanced diagnostic infrastructure, multidisciplinary approach, and strict adherence to clinical guidelines, which ensured the reliability and validity of the data collected. The setting provided a controlled environment for the observation of clinical practices and patient outcomes across various departments.
Study Population:
The study population comprised patients who presented to the hospital during the defined study period and met the inclusion criteria. The population was stratified into two groups based on age:
Pediatric group: Patients aged 0–18 years
Adult group: Patients aged 19 years and above.
This stratification enabled a comparative assessment of healthcare needs, treatment regimens, and diagnostic practices across different age groups. All participants included in the study had active clinical conditions requiring medical evaluation and treatment and were observed through their course of care without any deviation from standard hospital protocols.
Data collection:
Data were collected using a structured data collection form which included:
• Demographic Data: Age, gender, and presence of comorbidities.
• Clinical Data: Diagnosis, antibiotic prescribed, dosage, route of administration, and duration of therapy.
• Microbiological Data: Results from culture and sensitivity tests to determine antibiotic resistance patterns.
Data analysis:
Descriptive statistics were used to analyze the trends in antibiotic usage. Comparative analyses were performed using chi-square tests to evaluate differences in resistance rates between groups. Logistic regression models were employed to identify potential risk factors for antibiotic resistance. Data analysis was conducted using statistical software, and significance was determined at a p-value of <0.05.
This section presents the analysis of the data collected from 500 patients. The dataset comprises demographic, clinical, and microbiological data. Key calculations include the distribution of antibiotic use across different age groups, the percentage of patients with comorbidities, and the resistance rates among these groups
There are total 500 patients data out of which 240 are Female patients (48%) and 260 are Male patients (52%) out of which Pediatric patients are 162 (32.4%) and Adult patients are 338 (66.8%)
2. Antibiotic Usage Distribution Across Age Groups: Pediatric 35.20Adult 64.80
3. Percentage of patients with comorbidities are 50.8% and without comorbidities are 49.2%.
:4.Antibiotic Resistance Rates Among Age Groups:
-Pediatric:36.10%
- Adult: 63.90%
5. Culture Sensitivity Results:Out of total percentage 51.6% of culture sensitivity reports are found to be sensitive and 48.4% are resistant to the prescribed antibiotic in the medication.
6.Common Resistant Organisms Identified:
-Klebsiella:12.40%
-MRSA:9.60%
-E.Coli:9.40%
- Pseudomonas: 9.20%
Statistical Analysis:
|
Statistical Test |
Explanation |
|
-Used to compare categorical variables, such as the prevalence of antibiotic resistance between paediatric and adult patients. It determines if there's a significant association between groups. |
|
-Helps assess factors influencing antibiotic resistance while adjusting for confounding variables like age, comorbidities, or type of antibiotics used. |
|
-Used when comparing the means of a continuous variable (e.g., duration of antibiotic use) between two independent groups (paediatric vs. adult patients). Requires normal distribution. |
|
- A non-parametric alternative to the T-test, useful when the data is not normally distributed but still needs comparison between two independent groups. |
INCLUSION & EXCLUSION CRITERIA
Analysis of Resistance Rates Across Age Groups
This document presents the statistical analysis and graphical visualization of resistance and sensitivity rates across two age groups: Adults and Pediatrics. The objective is to determine whether there is a significant difference in resistance rates between these groups
1. Grouped Bar Chart
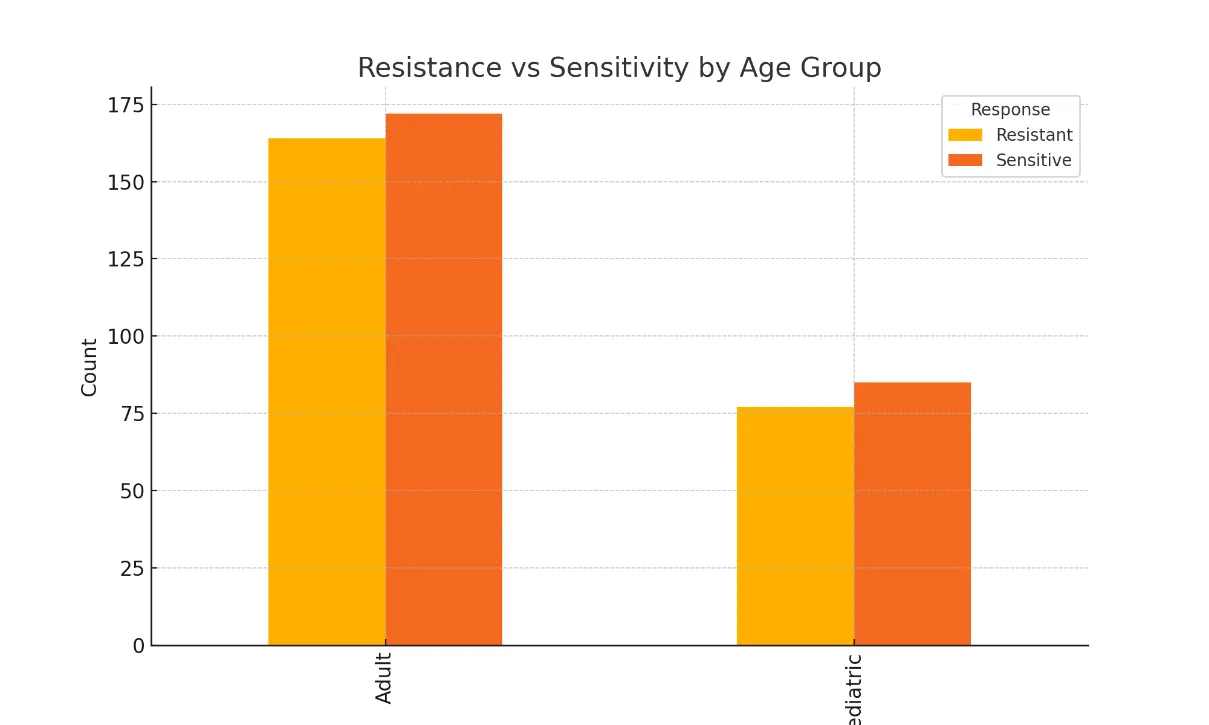
This bar chart compares the counts of resistant and sensitive cases between adults and pediatrics. Each age group has two bars representing the number of resistant and sensitive cases.
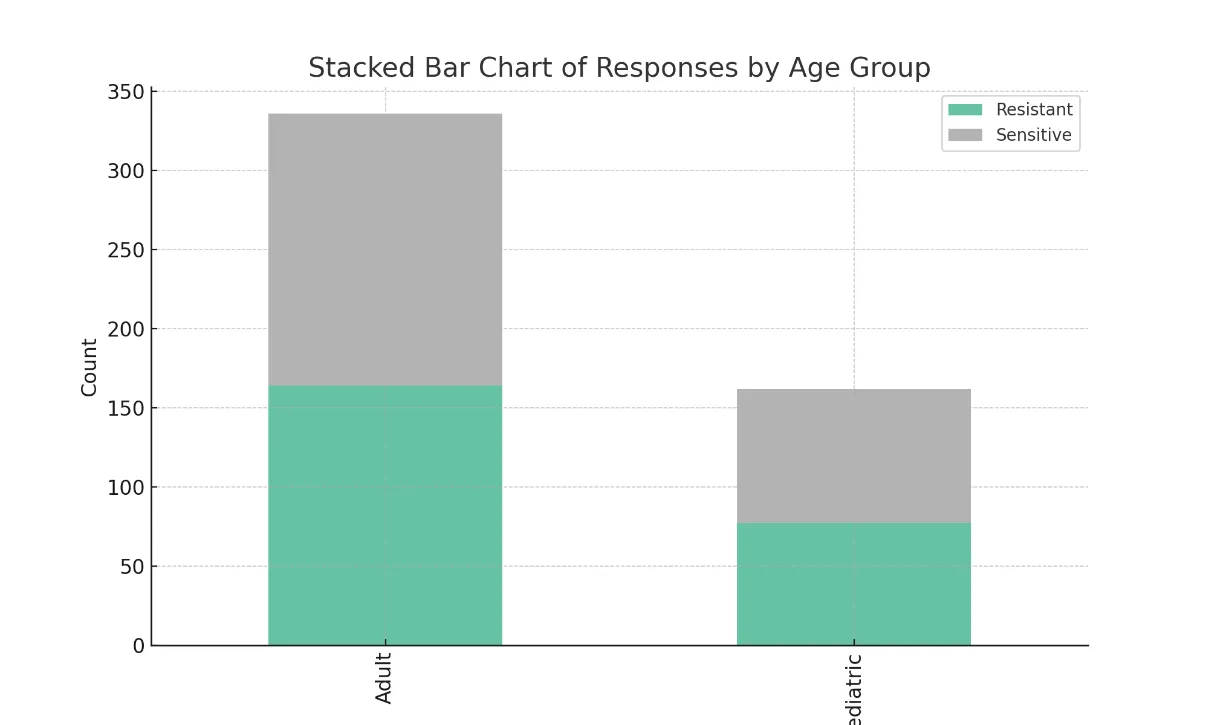
2. Stacked Bar Chart
This stacked bar chart shows the total number of cases in each age group, divided into resistant and sensitive sections. It helps visualize the proportion of resistance and sensitivity within each age group.
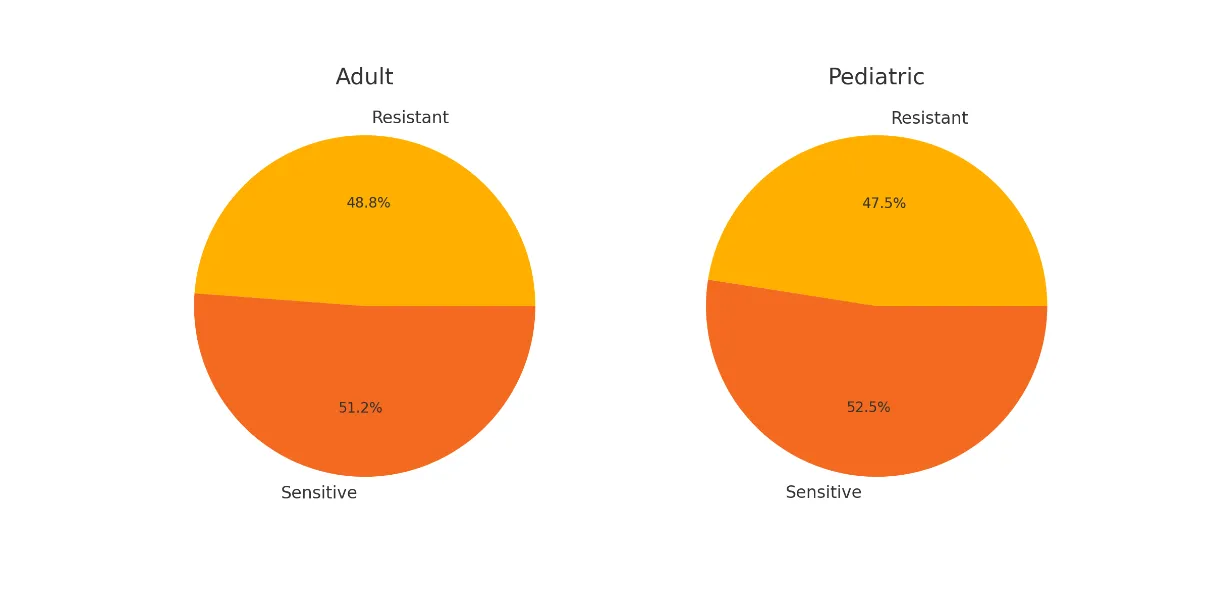
3. Pie Charts
Separate pie charts display the percentage distribution of resistant and sensitive cases for adults and pediatrics. The proportions are nearly identical, supporting the conclusion of no significant difference.
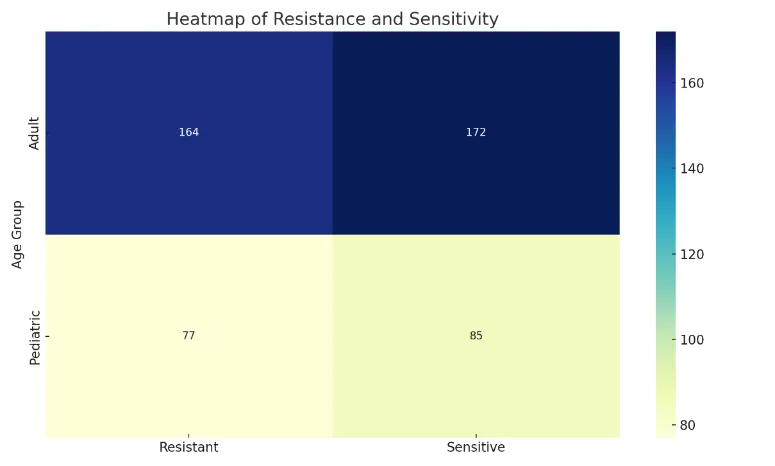
4. Heatmap
The heatmap provides a color-coded representation of resistance and sensitivity counts across age groups. Darker colors indicate higher frequencies. This is helpful for quickly identifying the most and least frequent outcomes.
CONCLUSION
Based on the Chi-square test, the calculated value (χ² = 0.074) with a p-value of 0.964 indicates no statistically significant difference in resistance rates between adult and pediatric age groups (p > 0.05). The visualizations confirm this result, as the proportions of resistant and sensitive cases are quite similar across both age groups.
A total of 500 patients were enrolled in this study.
A statistical analysis was carried out to compare the efficacy of different antibiotics using the Chi-square (χ²) test. The aim was to determine whether significant differences existed in their performance against the tested microbial strains. Antibiotics included in the analysis were Amoxicillin, Ciprofloxacin, Azithromycin, Vancomycin, Ceftriaxone, and Meropenem. The results of the pairwise comparisons are summarized below.
|
Comparison |
Chi-Square (X²) |
P-Value |
|
Meropenem vs Ceftriaxone |
2.3110 |
0.1280 |
|
Meropenem vs Ciprofloxacin |
2.1370 |
0.1440 |
|
Meropenem vs Vancomycin |
2.0790 |
0.1490 |
|
Meropenem vs Azithromycin |
1.8720 |
0.1710 |
|
Meropenem vs Amoxicillin |
1.7710 |
0.1830 |
|
Azithromycin vs Ceftriaxone |
0.0273 |
0.8690 |
|
Azithromycin vs Ciprofloxacin |
0.0996 |
0.9220 |
|
Amoxicillin vs Ceftriaxone |
0.0074 |
0.9320 |
|
Amoxicillin vs Ciprofloxacin |
0.0005 |
0.9720 |
|
Azithromycin vs Vancomycin |
0.0004 |
0.9850 |
|
Azithromycin vs Amoxicillin |
0.0000 |
1.0000 |
|
Vancomycin vs Amoxicillin |
0.0000 |
1.0000 |
|
Vancomycin vs Ciprofloxacin |
0.0000 |
1.0000 |
|
Vancomycin vs Ceftriaxone |
0.0000 |
1.0000 |
|
Ciprofloxacin vs Ceftriaxone |
0.0000 |
1.0000 |
DISCUSSION: -
The present study sought to assess and compare antibiotic usage and resistance trends among pediatric and adult patients, with and without comorbidities, in a tertiary care hospital. A prospective observational analysis involving 500 patients over six months was conducted to generate actionable data for improving antibiotic stewardship and guiding evidence-based prescribing practices.
1. Antibiotic Utilization Patterns
This study found that broad-spectrum antibiotics—specifically cephalosporins, macrolides, and fluoroquinolones [3]—were predominantly prescribed across both pediatric and adult populations. Notably, adults were more likely to be treated with carbapenems and fluoroquinolones, whereas pediatric patients were more frequently administered macrolides and amoxicillin-clavulanate. These observations underscore the differential prescribing preferences that arise from age-specific pharmacodynamics and comorbidity considerations.
These trends align with Alomar et al. (2019), who highlighted a pattern of higher empirical prescribing rates among adults, often driven by diagnostic uncertainty or delayed microbiological testing. The empirical reliance also reflects gaps in diagnostic support, which, if improved, could optimize antibiotic targeting and reduce unnecessary broad-spectrum use [10].
Furthermore, the findings support Patel et al. (2020), who emphasized that age significantly impacts antibiotic pharmacokinetics [1], influencing drug efficacy and safety profiles, which may partly explain prescribing preferences in different age groups.
2. Antibiotic Resistance Patterns
Despite distinct prescribing patterns, no statistically significant difference in overall resistance rates was observed between adult and pediatric groups (Chi-square, p = 0.964). Nonetheless, resistance was commonly noted for agents such as ceftriaxone, ciprofloxacin, and azithromycin, suggesting selective pressure due to frequent use. The data affirm the assertion by Hulscher et al. (2010) that inappropriate or prolonged antibiotic use [9], rather than patient age, is the principal driver of resistance development.
This convergence in resistance profiles across age groups emphasizes the need for antibiotic stewardship policies that transcend demographic boundaries and focus on antimicrobial de-escalation, timely switching to oral agents, and adherence to guidelines
Additionally, resistance trends observed in this study are in line with the global increase in multidrug-resistant organisms, particularly in hospital settings where empirical and prophylactic antibiotic use is high [2].
3. Role of Comorbidities
The presence of comorbid conditions—such as diabetes mellitus, chronic obstructive pulmonary disease (COPD), and renal impairment—was significantly associated with higher antibiotic resistance rates. These findings confirm the hypothesis that comorbidities independently contribute to increased susceptibility to multidrug-resistant infections. Mechanisms such as immune dysregulation, frequent healthcare contact, and polypharmacy likely underpin this relationship [8].
Our logistic regression analysis identified comorbidities as an independent predictor of resistance, further supporting the need for targeted interventions in patients with complex health profiles. These patients often receive prolonged or repeated antibiotic courses, which can disrupt the microbiota and promote colonization by resistant organisms [4].
Tailored antibiotic protocols, incorporating patient comorbidity profiles, are therefore essential. Notably, Gentry et al. (2018) observed that combination therapies in pediatric infections [6] showed better outcomes when adjusted for underlying health conditions, supporting the potential of personalized antibiotic strategies.
4. Antibiotic Stewardship Considerations
The findings of this study strongly support the implementation of structured Antibiotic Stewardship Programs (ASPs) in tertiary care settings. Rational prescribing anchored in culture and sensitivity data, strict adherence to the WHO AWaRe (Access, Watch, Reserve) classification, and formulation of age- and comorbidity-specific guidelines are critical to curbing resistance trends.
Evidence from Davey et al. (2017) and Roberts et al. (2018) substantiates the positive impact of ASPs, reporting reduced resistance rates [7], optimized antibiotic selection, shorter hospital stays, and lowered healthcare costs. Additionally, the integration of educational interventions for prescribers and the use of electronic decision-support tools have been effective in enhancing guideline adherence [10] [9].
Given the high empirical prescription rates in our study, embedding real-time microbiological diagnostics and providing feedback mechanisms for prescribers can facilitate a shift towards evidence-based antibiotic use. This is particularly critical in pediatric wards, where overuse of broad-spectrum agents may affect developmental immunological processes and increase future resistance risk.
SUMMARY:
This prospective observational study aimed to compare patterns of antibiotic usage and resistance between paediatric (0–18 years) and adult (19+ years) patients, with and without comorbidities, in a tertiary care hospital over a six-month period. The study included 500 patients, using demographic, clinical, and microbiological data to evaluate antibiotic prescribing trends and resistance profiles.
Key Findings:
Statistical methods like Chi-square, t-tests, and logistic regression were employed to analyse data, identify trends, and test for significant differences.
CONCLUSION
This study underscores the urgent need for refined antibiotic stewardship in tertiary care settings. Despite differing prescribing patterns, resistance rates were statistically similar between paediatric and adult groups, emphasizing that factors beyond age—such as comorbidities and empirical prescribing—play a more critical role in resistance development.
Key takeaways include:
The study supports the implementation of targeted Antibiotic Stewardship Programs (ASPs) and advocates for continued research through multicentric, longitudinal studies. Strengthening diagnostic capacity, enhancing clinician awareness, and promoting rational antibiotic practices will be vital steps in combating the rising threat of antimicrobial resistance.
FUTURE DIRECTIONS
The findings from this prospective observational study offer critical insights into antibiotic usage and resistance patterns across pediatric and adult populations in a tertiary care setting. However, the dynamic nature of antimicrobial resistance (AMR) necessitates continued research. The following future directions are proposed to build upon the current study :
1. Expansion of Study Scope and Duration
Multicentric Studies: Conduct similar studies across multiple tertiary care hospitals in different geographical regions to validate findings and identify region-specific resistance patterns.
2. Development of Risk Stratification Models
Individualized Therapy: Use stratification models to personalize antibiotic regimens, especially in patients with comorbidities or previous hospitalizations.
3. Implementation of Real-Time Antibiotic Stewardship Programs
Clinical Decision Support Systems (CDSS): Deploy electronic systems that integrate culture reports, resistance data, and prescribing history to guide clinicians in real-time.
Stewardship Rounds: Conduct regular multidisciplinary rounds involving pharmacists, microbiologists, and infectious disease specialists to audit and refine antibiotic prescriptions.
4. Focus on Pediatric and Comorbidity-Specific Guidelines
Pediatric-Specific Protocols: Develop antibiotic prescribing guidelines tailored to pediatric pharmacodynamics and microbial flora.
Management of High-Risk Comorbidities: Create specialized protocols for patients with diabetes, COPD, renal impairment, and immunocompromised states to mitigate resistance development.
5. Educational and Behavioral Interventions
Healthcare Provider Training: Organize periodic workshops and CMEs to update clinicians on local resistance trends and stewardship best practices.
Public Awareness Campaigns: Promote rational antibiotic use through patient education initiatives to reduce self-medication and enhance compliance.
6. Evaluation of Clinical Outcomes and Cost-Effectiveness
Outcome-Based Research: Assess how improved antibiotic prescribing impacts clinical outcomes such as treatment success rate, hospital stay duration, and readmission rates.
Economic Evaluation: Analyze the cost-effectiveness of stewardship programs and molecular diagnostics in preventing multidrug-resistant infections.
REFERENCES


Gauri There*, Prisha Naidu, Abhishek Jha, Isha Vadnere, Swati Sandhan, Comparative Assessment of Antibiotics Use as Well as Resistance in Paediatric and Adult Patients with And Without Comorbidities in Tertiary Care Hospital – A Prospective Observational Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 1639-1652. https://doi.org/10.5281/zenodo.21263934
 10.5281/zenodo.21263934
10.5281/zenodo.21263934