
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Rayat Bahra Institute of Pharmacy, Hoshiarpur, Punjab, 146001.
In the past few years, Three-dimensional (3D) printing, commonly referred to as additive manufacturing, has been acknowledged as having a significant potential to revolutionize respiratory treatment. With a primary focus on customization, the paper addresses the use of 3Dimensional printing technology in respiratory disease research and treatment. Recently, it has been acknowledged that additive manufacturing, often known as three-dimensional (3D) printing, has the potential to revolutionize respiratory therapy. The potential applications of various 3Dimensional printing processes, like bioprinting, stereolithography, selective laser sintering, and fused deposition modelling in the development of drug delivery systems, respiratory scaffolds, respiratory devices, and models are also explored in this review. The usage of 3Dimensional printed lung/airway models for preclinical studies, surgical planning, as well as the optimization of aerosol drug delivery is discussed. In addition to this, the recent advances in bioprinting techniques for building functional lung tissue constructs and disease models are also discussed. Even as these advances have been made, issues of material biocompatibility, intricacy of lung configurations, scaling issues, and regulatory issues still need to be addressed. In summary, the 3Dimensional printing technique presents an opportunity for an expanded field of precise medicine in pulmonary healthcare, providing the potential for more effective results in terms of therapy, efficiency in drug delivery, and an increased awareness of respiratory health issues.
According to the World Health Organization (WHO), breathing-related diseases claim the lives of over four million people each year, and by 2030, chronic obstructive pulmonary disease (COPD) alone is anticipated to come in third. Leading to a cause of death globally. The only treatment available to patients with end-stage respiratory conditions is tissue transplantation. The lack of available donor organs and serious transplant-related risks like blood clots, infections, and implant rejection are disadvantages of this approach. In order to create implantable tissues, researchers concentrated on tracheal and lung engineering.123 Respiratory disorders like occupational lung disease, pulmonary arterial hypertension, sleep disorders, asthma, and tuberculosis have
all had significant effects on the worldwide standard of life and the economy. 4 Emerging techniques for designing living tissue structures show significant potential in the previously mentioned components for the treatment of respiratory illnesses.5 Because of advancements in biomaterials, biotechnology, and manufacturing technology, we can now produce live tissue constructs that mimic the cellular composition, anatomical characteristics, and biological functions of the lungs and airways. Lung and tracheal replacements made with 3D printing are moving from the lab to the clinic. Tracheomalacia was treated with the use of the 3D-printed extracellular tracheal stent.67 In the pharmaceutical industry, technology is continuously developing, providing new options for fulfilling the needs of customized medication therapy. As technology advances, three-dimensional (3D) printing technology will have various applications for the production of patient-specific drug delivery devices (DDD) and dosage forms.8
Patients will be guided by personalized medicine to take the right medication at the ideal time and dosage.9 Researchers have been looking into cutting-edge methods of customized medicine, such as genetic profiling, pharmacogenomics, molecular diagnostics, artificial intelligence (AI), and three-dimensional printing (3DP).103D printing may help us understand the lungs complicated anatomy, physiological systems, cell relationships, and pathophysiology of pulmonary illnesses. This method can therefore be very helpful for the creation of new therapeutic targets, medications, and equipment for the treatment of lung diseases.11An outline of the use of 3D printing in the diagnosis and treatment of pulmonary conditions, as well as in the development and assessment of inhaled medications. It has been established that 3D-printed models are a useful aid for surgical planning challenging patients; nevertheless, these findings need to be validated by prospective multicentre trials. 3D printing is pre-surgical planning and simulation of difficult circumstances 12. There is increasing evidence based on randomized controlled trials and multicenter studies, even though case reports and case series make up the majority of the current research on 3D printing. By using 3D-printed models to reduce operating room time and duration of stay, this retrospective study highlights the incorporation of 3D printing technology into clinical practice and its effects on patient care.Furthermore, adopting 3D-printed models leads to lower 30-day readmission and mortality rates.13
1.1 History:
In the 1980s, Additive manufacturing is an alternative term for name for three-dimensional (3D) printing, was developed as a means of industrial prototyping.Additive manufacturing, commonly referred to as three-dimensional (3D) printing, began as an industrial prototyping tool in the 1980s. Driven by the need for specialized drug delivery systems related to the paradigm shift toward personalized treatment, it entered the pharmaceutical industry in the early 2000s. In contrast to conventional manufacturing, 3D printing enables layer-by-layer production, offering exact control over the dosage, form, release kinetics, and spatial distribution of medications—all crucial for tailoring treatments to the specific requirements of each patient.14,15 In 2015, Aprecia Pharmaceuticals' first 3D-printed oral tablet using ZipDose® technology, Spritam® (levetiracetam), was approved by the FDA, signaling a significant advancement in pharmaceutical 3D printing. This significant event validated 3D-printed dosage forms' regulatory acceptability and sparked further investigation into more sophisticated delivery systems.16,17 For the treatment of TB, pulmonary fibrosis, and chronic obstructive pulmonary disease (COPD), inhalation therapy is necessary. On the other hand, standard inhalation devices usually lack customization, inadequate deposition, and inconsistent dosage administration. Researchers looked into 3D printing as a method for creating patient-specific inhalers and inhalable particles because of these challenges 18,19. Aerosolizable microparticles, customized dry powder inhalers (DPIs), and smart inhalation devices have been made possible by advancements in 3D printing technologies since the late 2010s. These technologies include fused deposition modelling (FDM), inkjet printing, selective laser sintering (SLS), and binder jetting. It is particularly advantageous in paediatric and geriatric populations with different lung function levels that these systems can be tailored to the individual's respiratory physiology, including lung volume and airflow patterns 20 21 In the field of pulmonary medicines, 3D printing is now seen as an innovative technology,with the potential to revolutionize treatment by enabling on-demand, site-specific, and patient-tailored inhalation therapy. 21
2. PULMONARY ANATOMY AND PHYSIOLOGY:
As the basic organs of the respiratory system, the lungs' primary job is to make it easier for gases from the surrounding air to enter the bloodstream. After passing via the alveoli and into the capillary network, oxygen enters the arterial system and finally permeates tissue.22The nose, oropharynx, larynx, trachea, bronchi, bronchioles, and lungs are the main components of the respiratory system. In the lungs, distinct lobes divide into more than 300 million alveoli. The alveoli are the primary site of gas exchange 23 The main breathing muscle, the diaphragm, is the phrenic nerve innervates it. The inspiratory muscles called external intercostals become more active during physical activity or respiratory difficulty.24
2.1 Structure and function of lungs and airway:
2.1.1 Airway: The airway, which is the key element within the respiratory system, possesses a distinct anatomical structure that comprises the trachea and bronchi. The trachea splits into left and right bronchi close to the upper border of the fifth thoracic vertebra after starting at the bottom edge of the larynx's cricoid cartilage. The secondary and tertiary bronchi connect the left and right major bronchi to the lungs, respectively.25 The airway's primary tasks are breathing, foreign body clearance, and respiratory regulation.26 The airway's ventilatory function is coordinated by a number of factors. Maintaining the health of the airway cavity is largely dependent on airway cartilage. Smooth muscle and fibrous tissue usually close the cartilaginous gap and the airway's posterior wall to prevent gas from leaking into the surrounding tissue. The epithelium of mucosa eliminates foreign objects and shields the airway from airborne pathogens. Moreover, immunity and respiratory control are controlled by the immune system and the submucosal nerve of the airway, respectively.27
2.1.2 Lung: Comprising the lung parenchyma and interstitium, the lung is a vital respiratory organ in humans. Alveoli are found within the pulmonary parenchyma, and the alveoli are surrounded by connective tissue, microvascular, and lymphatic vessels in the lung interstitium.28The lungs are primarily responsible for gas exchange and immunity in the respiratory system. The lungs major work is to promote gas exchange. The alveoli allow oxygen from the surrounding environment to enter the bloodstream. Carbon dioxide from tissue metabolism exits the body via the lungs. The lung vasculature is designed to facilitate these functions. The lung parenchyma emerges from the intricate branching of the air passages. The lungs' complex neurological control maintains adequate regulation of respiratory function, including airway size, ventilation, and defensive reflexes.29
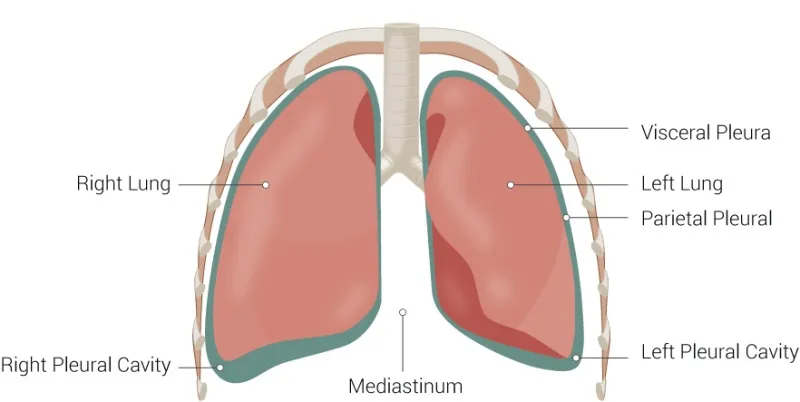
Fig. 1 Anatomy of lungs
2.1.3 Cells of the airway and lung:
Table.1 Cells of the airway and lung 30-38
|
Cell Type |
Location |
Primary Functions |
Relevance to Inhalable Drug Delivery |
|
Ciliated Epithelial Cell |
Trachea, Bronchi, Bronchioles |
Mucociliary clearance: move mucus upward. |
Drug residence time is affected, which is relevant in mucoadhesive formulation. |
|
Goblet Cells |
Trachea, Bronchi |
Secrete mucus to trap particles and pathogens. |
Mucus may hinder drugs; formulation must consider penetrating ability. |
|
Club (Clara) Cells |
Terminal Bronchioles |
Detoxification; surfactant secretion, and epithelial repair |
Targetable in bronchiolar diseases; responsive to oxidative and inflammatory stress |
|
Basal Cells |
Trachea, Bronchi |
Stem-like; regenerate epithelial lining |
Involved in tissue repair; relevance in chronic airway disease |
|
Neuroendocrine Cells (PNECs) |
Airway epithelium (rare) |
Sense oxygen, secrete neuropeptides |
Emerging target in inflammatory and fibrotic lung diseases |
|
Type1 Alveolar Cells (AEC 1) |
Alveoli |
Thin, flat; gas exchange |
Facilitate systemic absorption; passive uptake of small molecules |
|
Type 2 Alveolar Cells (AEC 2) |
Alveoli |
Surfactant secretion; progenitor for AEC 1 |
Interact with surfactant-modified drug carriers, crucial in ARDS. |
|
Alveolar Macrophages |
Alveolar surfaces |
Phagocytosis; immune defence |
Can clear or internalize inhaled particles; key target for infection control |
|
Dendritic Cells |
Airways and alveoli |
Antigen presentation; immune modulation |
Useful in inhalable vaccines and Immunotherapeutics |
|
Mast Cells |
Submucosa of airways |
Mediate allergic response, histamine release |
Targeted in anti-asthmatic inhalers |
|
Fibroblasts |
Lung interstitium |
Produce extracellular matrix; wound healing |
Key in fibrotic remodelling; target for anti-fibrotic therapies. |
3. 3D PRINTING FOR PULMONARY DRUG DELIVERY:
Attempts have been attempted to recreate the structure and functions of the alveoli in order to research gas exchange interactions, establish lung illness models, and conduct drug testing and toxicological investigations. The most difficult aspect of achieving this is simulating the complicated cell makeup in a thin layer while yet providing a supportive microenvironment. Furthermore, it is challenging to simulate the flexibility of the tissues and gas permeability across the membrane.39
3.1 Benefits of 3D Printing for Pulmonary Drug Delivery:
3.1.1 Personalized Airway Stents :3D printing allows for stents suited to each patient's unique airway architecture.
• Patient-specific stents can prevent problems such as migration, improve quality of life, and lessen the need for frequent replacement.
• 3D airway models enhance preoperative planning and training for airway stenosis, making endoscopic surgery safer and more successful.
3.1.2 Enhanced Surgical Planning: The 3D-printed lung models are based on CT scans and allow the surgeons to have a better understanding of the complex pulmonary anatomy (blood vessels, bronchi) in 3D, which is very helpful in difficult lung resections and bronchial surgery.
The application of 3D models has been shown to decrease the time of surgery and may even decrease the complications of surgery.
3.1.3 Education, Simulation, and Patient Communication: The application of 3D models for lungs and airways is of great benefit to surgeons, students, and patients. A tangible model is also very helpful for patients to understand their condition and the impending surgery, which is very helpful for informed consent and decision-making.
3.1.4 Resource Efficiency & Rapid Prototyping: 3D printing (additive manufacturing) enables rapid prototyping, which accelerates the development of new stent designs or devices.40
4. TYPES OF 3D PRINTING TECHNOLOGIES FOR PULMONARY:
4.1 Fused Deposition Modelling (FDM): A 3D printing technique called fused deposition modeling (FDM) makes use of thermoplastic filaments that are melted and extruded layer by layer. Consumer and industrial equipment frequently uses FDM, a rapid prototyping process, because of its affordability and ease of usage. Thermoplastic materials are deposited layer by layer using FDM technology to produce three-dimensional objects. FDM is a very adaptable technology that has been used in many different industries, including the aerospace industry for the manufacturing of lightweight materials, the medical business for the manufacture of implants and prostheses, and the educational sector for prototype and design applications.41 The foundation of the FDM manufacturing process is the melting of raw materials and their subsequent shaping. Wrapped around a roll and propelled by a drive wheel, the filament is heated to a semiliquid state in a temperature-controlled nozzle head.42Layer-by-layer structural components are produced by the nozzle's effective emission and guidance of materials in extremely thin layers. The layer outline that the CAD program specifies is followed by the FDM work system.43The few processing parameters that affect the mechanical properties of the printed components are the filament orientation, diameter, and layer thickness.44
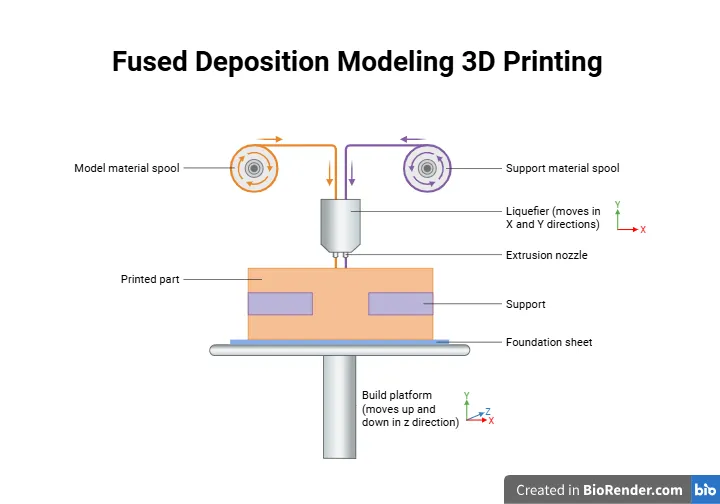
Fig 2: Fused Deposition Modelling
The primary material in the FDM process is the filament, which is typically made of pure polymer with a low melting point.[54] The filament can be made by moulding pellets or raw materials from polymeric materials. situations, the strength of the filament may need to be increased.45 Polymer filament is classified into two types: pure polymer filament and composite filament. The pure polymer filament is totally manufactured from a polymer compound without any additional solutions. 46The parameters influencing the printing process are separated into two categories: FDM machine parameters and working parameters. The machine's settings are bad temperature, nozzle temperature, and nozzle diameter. In contrast, working parameters include raster angle, raster width, build orientations, and so on, and these parameters are normally inputted in the slicing process using the software before the design and work parameters are uploaded into the FDM machine. 48,49
4.2 Stereolithography (SLA):
One of the most accurate and popular 3D printing technologies, stereolithography (SLA) uses a laser to cure liquid resin into solid layers, producing high-resolution models with complex details. SLA is highly preferred for applications that require smooth surfaces and fine features, making it perfect for the consumer electronics, medical, and aerospace industries.50Stereolithography (SLA) has completely changed the creation of customized pulmonary medication delivery systems. Drug carriers and inhalers that improve drug deposition and therapeutic efficacy in the lungs. According to recent research, SLA can be successfully combined with other technologies, including spray drying, to create inhalable compositions with enhanced aerodynamic qualities and regulated release profiles.51A laser is used in stereolithography, an additive manufacturing technique, to cure photosensitive resin and harden it layer by layer. A digital design file, often a CAD model, is the first step in the process. It is then divided into thin layers. The resin surface is exposed to a laser beam, which causes the resin to solidify where it strikes it. Until the part is completely created, this curing process keeps going.52SLA uses liquid resin, resulting in smoother finishes and considerably finer details. In order to selectively harden the material, the SLA printer usually uses a build platform that is submerged in the resin tank. The laser scans each layer.53
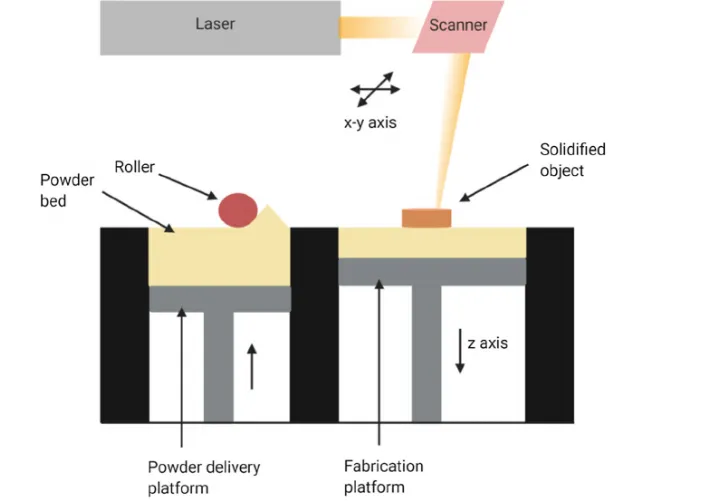
Fig3. Stereolithography (SLA)
4.3 Selective Laser Sintering:
Selective Laser Sintering (SLS) is a powder bed fusion-based 3D printing technique that allows for the creation of customized dry powder inhalation systems with controlled porosity and particle shape. By modifying printing conditions, SLS can create inhalable carriers and devices that are ideal for targeted lung deposition and prolonged medication release.54 SLS is quite good at creating devices out of a variety of polymers, but it is limited in its ability to work with ceramics and composite powders. This chapter covers in detail the potential of SLS technology in the production of biomedical devices, including a variety of materials, as well as its utilization in tissue engineering, medical implants, anatomical models, and drug delivery systems. Powder bed fusion 3D printing includes selective laser sintering (SLS), which employs a laser beam to heat powder particles and fuse them together at their surfaces to produce solid objects. Nowadays, industrial production of ceramic, metal, and plastic items uses 3-dimensional printing using selective laser sintering (SLS).55
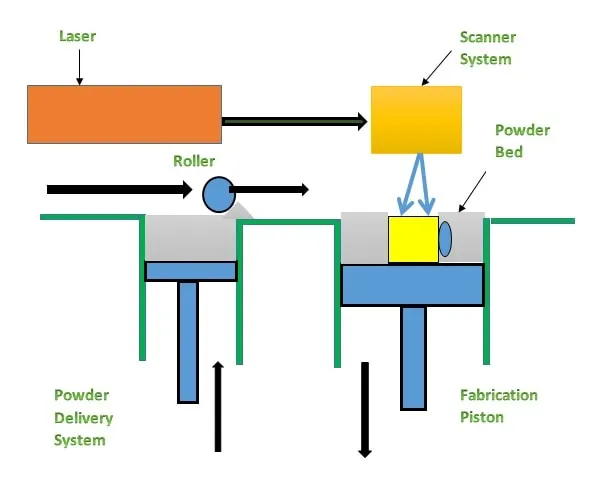
Fig4.Selective Laser Sintering 3D Printer
4.3.1 Components of Selective Laser Sintering 3D Printer:
Components of a 3D printer using selective laser sintering:
4.3.1.1 Laser: This powerful laser melts and fuses particles together.
4.3.1.2 Scanning System: After the laser is precisely aimed at the desired location, this system tracks the geometry of each layer.
4.3.1.3 Build Chamber: This is where the powdered material is stored.
4.3.1.4 Powder Delivery System: This system is used to transport and deliver the powder needed for each printing layer.
4.3.1.5 Powdered Form: This is the actual product in powdered form. The most popular material is nylon PA12.
4.3.1.6 Roller or leveller: For the subsequent printing cycle, a fresh layer of material is evenly distributed over the previously printed layer in the build chamber after being removed from the powder delivery system. 56
SLS uses a strong laser that accurately outline each layer in a bed of powdered material, often nylon.[64] This laser heats the powder particles and fuses them together to form powerful structures. The material is heated to a temperature lower than its melting point in order to use a laser to melt it, and the bed's height is changed such that the laser is centred on the newly created surface. The platform's loose powder offers assistance during the procedure.57 The next layer is deposited and fused after the powder bed is lowered by one layer each time. When a layer is complete, a powder recoater applies fresh powder evenly over the old layer while the build plate is slowly lowered. Because of its great accuracy, selective laser sintering typically uses layer thicknesses ranging from 50 to 200 microns. When they're done, the operator takes off and de-powders the prints. SLS offers the advantage of recycling a significant amount of the used powder, usually by mixing it with fresh powder. Making as many pieces as you can in a single print run, however, is a more efficient way to utilize the printing chamber's capacity.58
5. FUTURE PERSPECTIVE AND CHALLENGES:
The complex tissues such as airways and lungs are a major challenge in 3D bioprinting. There are many theoretical and technical hurdles that come in the way of its widespread use. This technology has the potential to bring about a revolution in the field of tissue engineering and the study of respiratory diseases.59
5.1 Challenges in theoretical bottleneck:
5.1.1 Theoretical challenges in bottleneck areas: The alveolar structure and function are theoretical bottlenecks. The alveoli in the lungs are very receptive suitable for gas exchange. The alveoli are thin-walled and are pre concise and sophisticated, requiring the right application of alveolar epithelial cells and capillary endothelial cells, considering functions such as surfactant secretion. They are very difficult to replicate.
5.1.2 Airway Branching and Cartilage Support: The airways are branching tubes lined with epithelial cells supported by cartilage. It is extremely difficult to properly replicate the branching pattern matching the right cells and adding cartilage support in bioprinting. To prevent rejection, the bioprinted lung and airway tissues should be immunocompatible with the recipient. The major theoretical challenge to be overcome is immunogenicity.60
5.1.3 Technological challenges Obstacle: Obstacles in Bioprinting with High Resolution: It is difficult to bioprint the airway and alveolar structures intricately with the current bioprinting technology because it lacks precision, has low resolution, and is not capable of bioprinting multiple cell types simultaneously.
5.1.4 In Mimicking Mechanical Properties: Lung tissues go through various kinds of stresses during respiration. Bioprinted items, in order to perform their function, would need to reproduce some mechanical properties-elasticity, compliance, and things like that-which current biomaterials cannot do.
5.1.5 Vascularization and Perfusion: Biologically vascularized bioprinting is extremely important to supply lungs with oxygen and nutrition. Therefore, printing functional blood vessels through such complex structures and connecting them with the host vascular network is an extremely challenging task.
5.1.6 Cell Sourcing and Differentiation Problems: Producing adequate quantities of cells such as alveolar epithelial cells, endothelial cells, and smooth muscle cells in available bioprinting while maintaining cell functions is difficult.
5.1.7 In Scaling-up and Clinical Translation: Translating the bioprinting method to the scaling up of large-sized lung and airway constructions that meet therapeutic objectives, while maintaining reproducibility and quality control, presents considerable technological obstacles.61
CONCLUSION
The design and construction of customized inhalable drug delivery devices for pulmonary disorders have seen a revolution because to three-dimensional (3D) printing. The exact control that 3D printing offers over drug dosage, particle geometry, and internal architecture, in contrast to traditional production methods, results in highly customizable formulations that can be tailored to the demands of specific patients and lung physiology. This accuracy allows for greater bioavailability, site-specific drug deposition, and improved treatment of long-term respiratory conditions such lung cancer, cystic fibrosis, asthma, and chronic obstructive pulmonary disease (COPD). The development of dry powder inhalers, porous microparticles, and biodegradable implants with adjustable drug release kinetics has demonstrated the great promise of several 3D printing processes, such as selective laser sintering (SLS), inkjet printing, and fused deposition modelling (FDM). Additionally, these technologies enable combination therapy and lower the frequency of doses by integrating various medications into a single device. Additionally, point-of-care and on-demand production are made easier by digital modelling and computer-aided design (CAD), which reduce waste and guarantee uniformity. Even with these developments, there are still issues with scalability, governmental licensing, and identifying printed biocompatible materials that are safe for inhalation. Overcoming these obstacles requires ongoing multidisciplinary research in biomedical engineering, pharmacology, and materials science. Finally, the creation of next-generation pulmonary drug delivery systems is made possible by 3D printing, which provides a creative and adaptable platform that opens the door to patient-centred, effective, and customized respiratory care. Therefore, 3D printing represents not merely a manufacturing tool but a transformative approach toward personalized medicine and advanced drug delivery.
REFERENCES
Ozbolat IT, Hospodiuk M. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials. 2016;76:321-343




Aniketa, Maninder Pal Singh, Gurpreet Kaur, Shallu Emerging 3D Bioprinting Techniques in Respiratory Medicine: Advances, Challenges, and Future Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 6968-6980, https://doi.org/10.5281/zenodo.20396554
 10.5281/zenodo.20396554
10.5281/zenodo.20396554