
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sigma Institute of Pharmacy, Sigma University, Bakrol, Vadodara 390019, Gujarat
Empagliflozin is a newer antidiabetic agent that acts by inhibiting the sodium–glucose co-transporter-2 (SGLT2), thereby promoting glucose excretion through urine. This mechanism improves glycemic regulation, decreases glucotoxicity, and enhances insulin sensitivity. Although initially developed for the management of type 2 diabetes mellitus (T2DM), empagliflozin has demonstrated significant additional benefits beyond glucose control. Clinical studies have highlighted its strong cardioprotective and nephroprotective effects, including reduced rates of heart failure hospitalization, cardiovascular mortality, and progression to end-stage renal disease. The drug effectively lowers fasting and postprandial blood glucose levels, HbA1c, and average daily glucose, while also contributing to weight reduction. Empagliflozin is generally well tolerated; however, its use is limited in patients with severe renal impairment (GFR < 30 mL/min/1.73 m²) or hypersensitivity reactions. Common adverse effects include hypotension, genital fungal infections, urinary tract infections, and rare cases of ketoacidosis.
Empagliflozin is an orally administered antihyperglycemic agent that entered clinical practice in 2014. It is classified as a sodium–glucose co-transporter-2 (SGLT2) inhibitor, a drug class developed specifically for managing type 2 diabetes mellitus (T2DM). SGLT2 plays a key role in renal glucose handling, as it is primarily responsible for glucose reabsorption from the glomerular filtrate in the proximal tubules. Targeting this transporter offers a novel therapeutic approach for controlling hyperglycemia in T2DM. Empagliflozin acts by effectively inhibiting renal glucose reabsorption, leading to increased glucose elimination through urine. Compared with other SGLT2 inhibitors that are currently approved or under investigation, empagliflozin demonstrates greater selectivity for SGLT2 than for sodium–glucose co-transporter-1 (SGLT1).
MECHANISM OF ACTION OF EMPAGLIFLOZIN: [2]
Empagliflozin is a selective inhibitor of sodium–glucose co-transporter-2 (SGLT2), which is predominantly located in the proximal convoluted tubule of the kidney. Under normal conditions, SGLT2 is responsible for reabsorbing nearly 90% of the filtered glucose back into the bloodstream. By inhibiting this transporter, empagliflozin reduces renal glucose reabsorption, leading to increased glucose excretion in urine (glycosuria). This insulin-independent mechanism lowers plasma glucose levels without stimulating insulin release. The associated osmotic diuresis also contributes to mild reduction in blood pressure and body weight. Due to its high selectivity for SGLT2 over SGLT1, empagliflozin produces effective glucose lowering with minimal gastrointestinal effects.
INTRODUCTION TO DISEASE: [3]
Diabetes mellitus is a long-term metabolic condition involving disturbances in the metabolism of carbohydrates, fats, and proteins. The disorder is primarily characterized by an inadequate insulin secretion or an ineffective insulin response, leading to impaired utilization of glucose by body tissues. As a consequence, blood glucose levels rise above normal limits, resulting in persistent hyperglycaemia. Owing to this elevated glucose concentration in the blood, diabetes mellitus is commonly known as “sugar disease.” It represents the most prevalent endocrine disorder and typically develops due to an absolute or relative deficiency of insulin, or less frequently, due to reduced sensitivity of tissues to insulin action.
SYMPTOMS OF DIABETES MELLITUS:
PATHOPHSIOLOGY OF TYPE 2 DIABETES MELLITUS: [4]
Type 2 diabetes mellitus develops primarily due to reduced sensitivity of peripheral tissues to insulin. In the early stages, the pancreas compensates by increasing insulin secretion. Over time, continued metabolic stress leads to progressive beta-cell impairment. In addition, excessive glucose release by the liver contributes to elevated blood glucose levels, particularly in the fasting state.
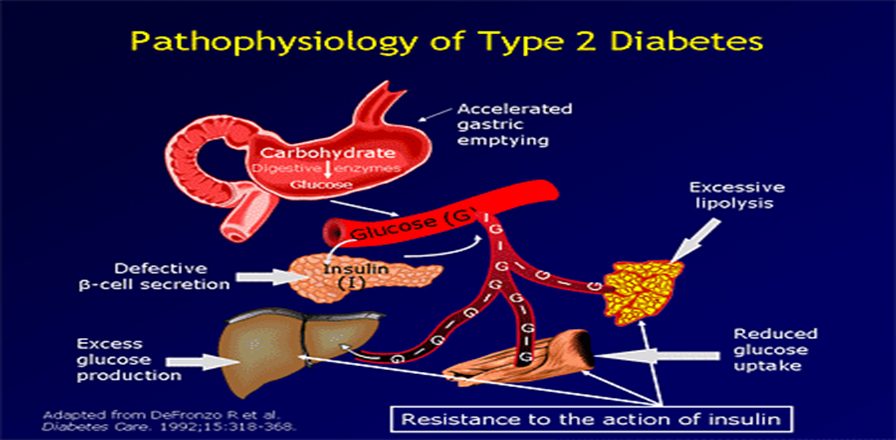
Figure 1: Pathophysiology of type 2 Diabetes [5]
DRUG PROFILE OF EMPAGLIFLOZIN:
Jardiance (empagliflozin) was first Initially approved by the U.S. Food and Drug Administration (FDA) on August 1, 2014
Table 1-Physiochemical properties of Empagliflozin [6-7]
|
Sr. No |
Name |
EMPAGLIFLOZIN |
|
1) |
IUPAC Name |
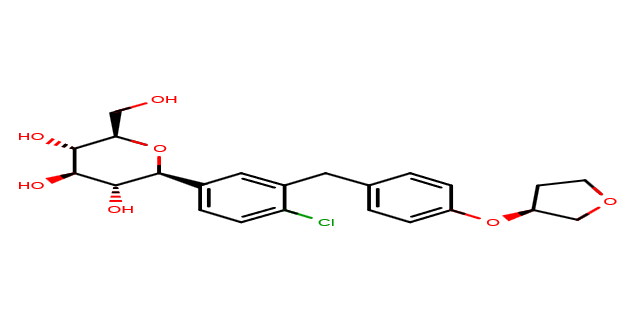
(2S,3R,4R,5S,6R)-2-[4-chloro-3-[[4-[(3S)-oxolan-3-yl]oxyphenyl]methyl]phenyl]-6-(hydroxymethyl)oxane-3,4,5-triol |
|
2) |
Class |
Sodium–glucose co-transporter 2 (SGLT2) inhibitors |
|
3) |
Category |
Anti- diabetic |
|
4) |
CAS no |
864070-44-0 |
|
5) |
Molecular Formula |
C23H27ClO7 |
|
6) |
Structural Formula |
|
|
7) |
Molecular Weight |
450.9 g/mol |
|
8) |
Official status |
Approved by the U.S. FDA, August 1, 2014. |
|
9) |
Appearance |
White to off-white crystalline powder |
|
10) |
Physical state |
Solid |
|
11) |
Solubility |
Very slightly soluble in water |
|
12) |
Pka |
12.5 (strongest acid), -3 (strongest basic) |
|
13) |
Melting Point |
150–153?°C |
|
14) |
Partition coefficient (log P) |
1.7–1.8 |
|
15) |
Mechanism Action |
Empagliflozin is a selective inhibitor of the sodium-glucose co-transporter 2 (SGLT2), which is primarily expressed in the proximal tubules of the kidneys. Under normal physiological conditions, SGLT2 reabsorbs approximately 90% of filtered glucose from the renal tubular lumen back into the bloodstream. By inhibiting SGLT2, empagliflozin reduces glucose reabsorption, leading to increased urinary glucose excretion (glucosuria). This process lowers plasma glucose levels independently of insulin secretion or action, making it effective in the management of type 2 diabetes mellitus. Additionally, the induced glucosuria results in mild osmotic diuresis, contributing to modest reductions in body weight and blood pressure. |
|
16) |
Uses |
Type 2 Diabetes mellitus |
LITERATURE REVIEW OF EMPAGLIFLOZIN:
Table 2 UV spectroscopic method of empagliflozin
|
Sr no. |
Title |
Description |
Ref |
|
1. |
Development validation and forced degradation studies of empagliflozin using uv spectroscopy in a comprehensive approach |
Solvent- methanol Wavelength- 223 nm Linearity- 2–10 µg/ml |
8 |
|
2. |
Simultaneous method development and validation of uv spectroscopic method for the estimation of empagliflozin and sitagliptin in bulk dosage form |
Solvent- methanol / water diluent Wavelength- 224 nm (emp) / 267 nm (sit) Linearity- 5–25 µg/ml (emp) |
9 |
|
3. |
Development and validation of uv spectrophotometric method for simultaneous estimation of empagliflozin and metformin hydro-chloride in combined dosage form
|
Solvent- methanol Wavelength- 224 nm (emp), 233 nm (met); also 266 nm isobestic used Linearity- 0.1–25 μg/ml (emp); 0.5–25 μg/ml (met) |
10 |
|
4. |
Spectrophotometric simultaneous determination of empagliflozin and metformin in combined tablet dosage form by absorbance corrected method, area under curve method, and dual wavelength spectrophotometry. |
Solvent- methanol (and water) Wavelength- 224 nm (emp) & 232 nm (met) Linearity- 2–10 μg/ml (emp); 4–20 μg/ml (met) |
11 |
Table 3 HPLC method of empagliflozin
|
Sr no. |
Title |
Description |
Ref |
|
1. |
Development And Validation of Analytical Method for Simultaneous Estimation Of Empagliflozin And Metformin By Rp-Hplc |
Mobile Phase- Methanol: Acetonitrile (75:25 V/V) Stationary Phase- X-Bridge C18 (4.6 × 150 Mm, 5 µm) Wavelength- 260 Nm Flow Rate- 1.0 Retention Time- ~14 Min Linearity- R² > 0.999 For Both |
12 |
|
2. |
Development And Validation Of Rp-Hplc Method For The Simultaneous Estimation Of Empagliflozin And Metformin Hydrochloride In Bulk Drug And Tablet Dosage Form.
|
Mobile Phase- Methanol: Kh?Po? Buffer (60:40 V/V) Stationary Phase- Cosmosil C18 (250 × 4.6 Mm, 5 µm) Wavelength- 227 Nm Flow Rate- 0.8 Retention Time- Empagliflozin: 6.7 Linearity- Empagliflozin: 1–5 µg/Ml |
13 |
|
3. |
Validated Stability Indicating RP-HPLC Method For The Forced Degradation Study Of Empagliflozin. |
Mobile Phase- Ammonium Acetate: ACN (62:38) Stationary Phase- C18 RP Column (250 × 4.6 Mm, 5?µm) Wavelength- 265 Flow Rate- 1.0 Retention Time- EMP: ~5.3 Linearity- (R² ~0.998) |
14 |
|
4. |
Stability Indicating Method Development And Validation For Determination Of Metformin And Empagliflozin In Bulk And Pharmaceutical Dosage Form By RP-HPLC |
Mobile Phase- 0.1% OPA Buffer : ACN (60:40) Stationary Phase- Symmetry C18 (150 × 4.6 Mm, 5?µm) Wavelength- 230 Flow Rate- 1.0 Retention Time- MET: ~2.28; EMP: ~2.89 |
15 |
|
5. |
Stability-Indicating HPLC-DAD Method For The Determination Of Empagliflozin
|
Mobile Phase- Methanol/Acetonitrile/0.1% OPA 75:20:5 Stationary Phase- Poroshell EC?C18 (100 × 4.6 Mm, 4?µm) Wavelength- 222 Flow Rate- 1.0 Retention Time- EMP: ~2.54 Linearity-10–50?µg/Ml (R²=0.9990) |
16
|
|
6. |
Development And Validation Of Rapid Stability-Indicating High-Performance Liquid Chromatography Method For The Determination Of Linagliptin And Empagliflozin In Pure And Dosage Forms |
Mobile Phase- Phosphate Buffer: Acn (65:35, V/V) Stationary Phase- C18 Rp Column (150 × 4.6 Mm, 5?µm) Wavelength- 226 Flow Rate- 1.0 Retention Time- Emp: ~2.54 Linearity-10–50?µg/Ml (R²=0.9990) |
17 |
Table 4 HPTLC method of empagliflozin
|
Sr no. |
Title |
Description |
Ref |
|
1. |
Greenness assessment and stability-indicating hptlc method for the concurrent analysis of empagliflozin and metoprolol succinate in a novel combined oral formulation
|
Mobile phase- chloroform: methanol: toluene (3.0:2.5:4.5 v/v/v) Stationary phase- silica gel 60 f254 plates Wavelength- 222nm Concentration range- Emp: 100–600 ng/band; Meto: 500–3000 ng/band |
18 |
|
2. |
Stability indicating assay method for estimation of empagliflozin using hptlc |
Mobile phase- chloroform: toluene: methanol: methanolic acid (8:4:2:0.1 v/v/v/v) Stationary phase- silica gel 60 f254 Wavelength-222nm Concentration range- 100–700 ng/band |
19 |
Table 5 LC-MS method of empagliflozin
|
Sr no. |
Title |
Description |
Ref |
|
1. |
Development and validation of empagliflozin and linagliptin simultaneous estimation in rat plasma using freezing lipid precipitation and scx-spe assisted hplc–ms/ms method and its application in pharmacokinetic studies |
Stationary phase- reverse-phase c18 (bioanalytical) Mobile phase- spe clean-up + lc eluents (details in paper) Mass spectrometric detection- esi, mrm Linearity- empa: 25–1050 ng/ml; lin: 0.35–15 ng/ml |
20 |
CONCLUSION:
The collective evidence from these studies highlights empagliflozin as a widely investigated SGLT2 inhibitor with extensive applications in the management of type 2 diabetes mellitus. Recent research demonstrates the development and validation of robust analytical techniques, including UV-spectroscopy, HPLC, HPTLC, and LC-MS/MS, for the simultaneous estimation of empagliflozin with other antidiabetic agents such as metformin, sitagliptin, and linagliptin. Stability-indicating methods are emphasized across multiple studies, ensuring accuracy, precision, and reliability in both bulk drug and combined dosage forms. Additionally, forced degradation and greenness assessments indicate a growing focus on method sustainability and pharmaceutical quality control.
REFERENCES


Kiran Sharma, Mitali Dalwadi, Empagliflozin in Modern Diabetes Care: Future Directions in Patient Care, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 2399-2405. https://doi.org/10.5281/zenodo.18341280
 10.5281/zenodo.18341280
10.5281/zenodo.18341280