
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
¹ Department of Pharmacy Practice, JSS College of Pharmacy, Ooty, India
² Senior Consultant, Medical Oncology, Hemato-oncology and BMT, Gleneagles Hospital, Sholinganallur, Chennai, India
³ Clinical Lead and Senior Consultant, Medical Oncology, Gleneagles Institute of Oncology, Sholinganallur, Chennai, India
4 Clinical Pharmacology, Oncology, HCG Cancer Centre, Bengaluru, India
Background: Chemotherapy-induced nausea and vomiting is one of the most debilitating side effects of chemotherapy in cancer patients. This has a significant impact on quality of life and chemotherapy compliance in cancer patients. Despite various guidelines being formulated by different organizations such as ASCO, MASCC/ESMO, and NCCN, inappropriate antiemetic therapy is one of the commonly encountered drug-related problems. Materials and Methods: A six-month mixed prospective and retrospective observational study was conducted on 95 cancer patients undergoing chemotherapy in a tertiary care hospital. Emotogenic risk assessment was done using Hesketh classification. Result: Moderately emetogenic chemotherapy was more commonly prescribed, followed by highly emetogenic chemotherapy. The overall antiemetic drug prescription appropriateness was found to be low, and most of them were inappropriate. The overall guideline compliance was found to be low, and partial compliance was more than full compliance. The reasons for non-compliance were under-treatment, over-treatment, and inappropriate treatment duration. The commonly prescribed antiemetic drugs were ondansetron and dexamethasone, whereas the least prescribed antiemetic drugs were neurokinin-1 receptor antagonists. Gastric protection agents, particularly PPIs, were highly prescribed, and most of them were inappropriate. The commonly encountered antiemetic drug-related problems were inappropriate antiemetic drug selection, inappropriate use of gastric protection agents, and inappropriate treatment duration. Conclusion: It can be concluded that the gap between recommendations and practice is huge. Therefore, a clinical pharmacist should be involved, and a review of drug utilization should be done frequently.
Cytotoxic chemotherapy is a key part of cancer therapy, but it comes with several side effects. The most troubling side effect patients experience during chemotherapy is nausea and vomiting [1]. Chemotherapy-induced nausea and vomiting (CINV) poses a serious clinical issue. Despite progress in supportive care, CINV impacts up to 40% of patients [2]. If it is not managed, it can harm a patient’s quality of life. This often leads to a reduction or stop in chemotherapy due to these uncontrolled side effects. CINV may also cause complications like dehydration, electrolyte imbalances, and mucosal injuries such as Mallory-Weiss syndrome [3-5].
Preventing and managing CINV is vital for improving patient comfort and ensuring patients stick with their cancer treatment. However, a significant gap exists between clinicians’ perceptions and patients’ actual experiences, which often results in poor symptom control [6]. Studies show that underestimating the emetogenic potential of chemotherapy is one major reason antiemetic therapy fails [7]. CINV is divided into acute and delayed phases. The acute phase usually happens within 24 hours of chemotherapy, peaking in just a few hours [4,5]. The emetogenic potential of the chemotherapy regimen mainly determines the risk. However, patient-related factors, including age, gender, alcohol consumption, motion sickness history, and previous episodes of CINV, are also important in assessing risk [3,8,9]. CINV is an important issue in the management of patients with cancer, as it significantly affects the quality of life and the continuation of chemotherapy regimens [10-13]. CINV also has an economic impact on the healthcare system due to the increased healthcare costs associated with CINV [14-16].
To tackle this issue, several international organizations, including the American Society of Clinical Oncology and the Multinational Association of Supportive Care in Cancer, have released evidence-based guidelines for preventing and managing CINV. The guidelines stress the need to assess the risk of chemotherapy-induced nausea and to use combination antiemetic therapy based on the emetogenic potential of chemotherapy [17,18]. However, there is a problem with following these guidelines in clinical practice.
Apart from antiemetics, gastric protective agents, such as PPIs, are commonly used in oncology patients. Although PPIs are efficient in controlling acid-related diseases, their use has escalated significantly, sometimes in the absence of clear indications [19] . Research has documented a high incidence of inappropriate PPI therapy, which accounts for 50% of inpatient and outpatient populations [20]. Although PPIs are safe in short-term therapy, long-term or unnecessary use of PPIs has resulted in serious drug interactions, increased risk of infections, nutrient absorption, and renal and neurological problems [21].
Drug utilization evaluation is an important tool in the assessment of drug use and promotion of rational pharmacotherapy. This helps in the identification of irrational use of medication, including aspects such as the selection, dosage, duration, and interaction of the medication used [22].It is known that irrational use of medication and polypharmacy contribute to morbidity, mortality, and increased healthcare costs [23]. Even though various studies were carried out on the use of antiemetics and gastroprotective agents individually, there is limited information available on the concurrent assessment of both in the same setting.
Thus, the aim of the current study was to assess the appropriateness of antiemetic and gastric protective agent use, along with compliance with guidelines, in adult oncology patients undergoing chemotherapy. Such an approach is considered to be important to identify areas of current practice, thereby optimizing supportive care in oncology (Figure:1).
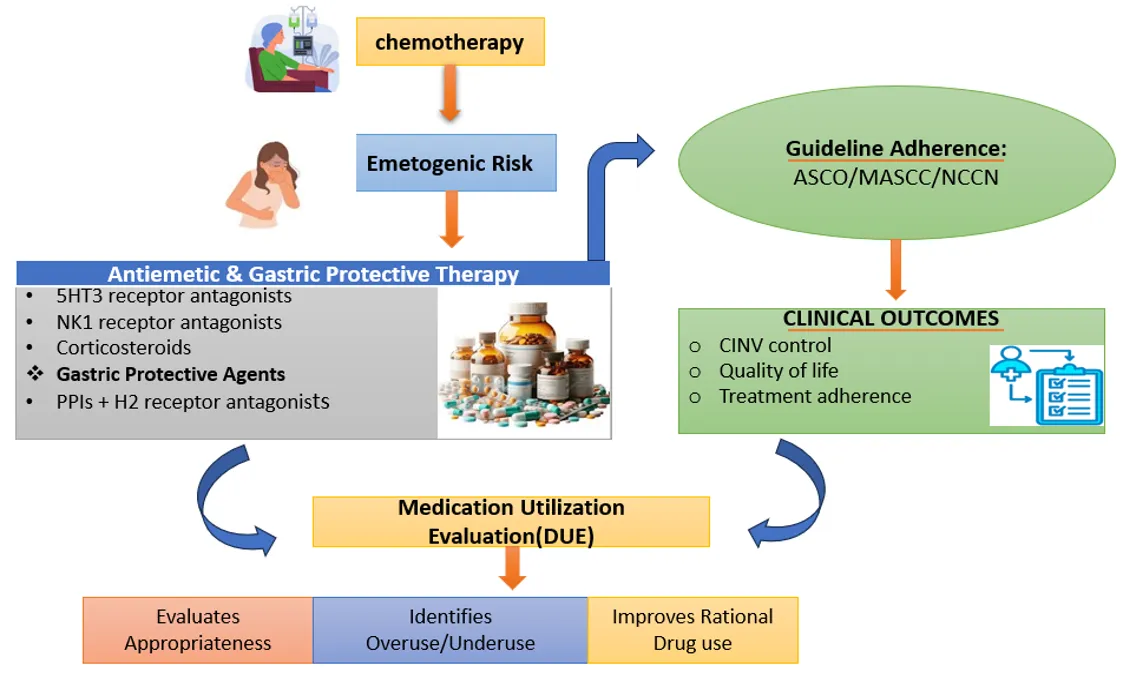
Figure 1: Overview of emetogenic risk assessment, supportive therapy, and guideline adherence in chemotherapy patients.
METHODS:
Study Design and Population:
The study was a mixed retrospective and prospective observational study conducted among adults with cancer and undergoing chemotherapy in a tertiary care teaching hospital setting in Chennai during 6 months. The Institutional Ethics Committee (Protocol ID: BMHR/2026/0163) approved the study. The study involved convenience sampling. The inclusion and exclusion criteria were used to select the participants. The research was conducted in two stages, where the retrospective study was performed in 2025 between September and December and the prospective study was performed in 2026 between January and February. Following the assessment process, the selection of research participants was done as per the inclusion and exclusion criteria. A sample of 95 patients was chosen to participate in the study.
Eligibility Criteria:
The selection of the participants was based on some inclusion and exclusion criteria. The respondents were adult patients older than 18 years, with any type of malignancy, undergoing chemotherapy, and were sampled in the study. Second, the patients who were on antiemetic agents and/or gastric protective agents (such as proton pump inhibitors or H₂ receptor antagonists) were also chosen to participate in the research. Nevertheless, only patients whose medical records were complete were included in the study in the retrospective section of the research. The patients were not included in the sample, which was considered to be under 18 years. Secondly, patients receiving radiotherapy, immunotherapy, or targeted therapy or patients admitted to the palliative care facility were not included in the study. In addition, patients whose medical records were incomplete or not available were not included in the study to provide the correct data.
Data collection procedure: –
Data collection for the current study was done using a combination of prospective and retrospective methods. In the retrospective approach, the data was collected from patient case records, chemotherapy records, and medication records. In the prospective approach, the data were collected by direct observation of patients and their prescription records during hospital visits. The data collected included patient demographics, the nature of the cancer and chemotherapy (limited to one identified malignancy), and the emetogenic risk factors associated with the chemotherapy. In addition to that, detailed records of the anti-emetic and gastric protectors used in the treatment were also noted.
Outcome Measures:
The classification of the emetogenic activity of the chemotherapy regimens was done according to the classification of Hesketh, where the chemotherapy agents are classified according to the amount of emesis the agent is capable of producing. It consists of five levels: >90% (Level 5, highly emetogenic), 60-89% (Level 4), 30-59% (Level 3), 10-29% (Level 2), and <10% (Level 1, minimally emetogenic). This classification was done based on analysis in terms of emetogenicity of chemotherapy regimens as highly emetogenic, moderately emetogenic, low emetogenic, and minimally emetogenic chemotherapy in terms of antiemetics.
Statistical Analysis:
Descriptive statistical analysis was used to analyze the collected data. Continuous variables were described as mean and standard deviation, and categorical variables were described in terms of frequency and percent. No statistical test was used.
RESULTS:
A total of 95 patients were included. Their mean age was 60.2 ± 11.5 years, ranging from 30 to 87 years. Patients aged >60 years constituted the majority (47.4%), followed by those aged 41–60 years (46.3%), and those aged 18–40 years (6.3%). Females accounted for 56.8%, and males accounted for 43.2% (Table 1).
Table 1. Baseline Demographic and Clinical Characteristics (n = 95)
|
Variable |
Category |
Percentage (%) |
|
Age Group (years) |
18–40 |
6.3 |
|
41–60 |
46.3 |
|
|
>60 |
47.4 |
|
|
Gender |
Female |
56.8 |
|
Male |
43.2 |
|
|
Type of Cancer |
Breast cancer |
28.2 |
|
Gastrointestinal cancer |
21.1 |
|
|
Gynecological cancer |
13.7 |
|
|
Hematological malignancy |
13.7 |
|
|
Genitourinary cancer |
9.5 |
|
|
Head and neck cancer |
5.3 |
|
|
Lung cancer |
5.3 |
|
|
CNS tumor |
2.1 |
|
|
Sarcoma |
1.1 |
|
|
Cancer Stage/Status |
Stage III |
1.1 |
|
Stage IV |
5.3 |
|
|
Metastatic disease |
21.1 |
|
|
Recurrent/relapsed |
7.4 |
|
|
Grade I |
5.3 |
|
|
Grade II |
13.7 |
|
|
Grade III |
7.4 |
|
|
TNM only reported |
29.5 |
|
|
Not available |
9.5 |
|
|
Emetogenic Risk |
High |
26.6 |
|
Moderate |
40.4 |
|
|
Low |
17.0 |
|
|
Minimal |
16.0 |
The most common type of cancer was breast cancer 28.2%, while gastrointestinal cancers accounted for 21.1%. Gynecological and Hematological cancers were 13.7% each, while other cancers were genitourinary, 9.5%; head and neck and lung 5.3%. With respect to disease status, The incidence of metastasis was 21.1%, followed by Grade II tumors, which accounted for 13.7%. TNM staging, unspecified, was recorded in 29.5% of cases, whereas Stage IV and Stage III cancers accounted for 5.3% and 1.1%, respectively (Table 1).
Out of the total 95 patients, the majority had at least one comorbidity. Comorbid conditions were present in approximately 78.7% of patients, while 21.3% had no documented comorbidities. The most common comorbid conditions were diabetes mellitus (66.7%) and hypertension (38.7%), followed by hypothyroidism (13.3%) and coronary artery disease (12%) (Table 2).
Regarding lifestyle factors, Most patients were non-drinkers (65.3%) and non-smokers (70.2%) ( Table 2).
A history of CINV was reported in 53.7% of patients, while 68.4% had no history of motion sickness. The most common type of chemotherapy was moderately emetogenic, accounting for 40.4%, while highly emetogenic, low, and minimal regimens were 26.6%, 17%, and 16%, respectively (Table 2).
Based on Hesketh classification, The most common type of chemotherapy was moderately emetogenic, accounting for 40.4%, while highly emetogenic, low, and minimal regimens were 26.6%, 17%, and 16%, respectively (Table 2).
Table 2. Comorbidities and Lifestyle Characteristics
|
Variable |
Category |
Percentage (%) |
|
Comorbidities (overall) |
Present |
78.7 |
|
Absent |
21.3 |
|
|
Common Comorbidities |
Diabetes mellitus |
66.7 |
|
Hypertension |
38.7 |
|
|
Hypothyroidism |
13.3 |
|
|
Coronary artery disease |
12.0 |
|
|
Dyslipidemia |
8.0 |
|
|
Other Conditions |
Anemia |
6.7 |
|
Acute cholangitis |
6.7 |
|
|
Asthma/COPD |
5.3 |
|
|
Stroke/CVA |
5.3 |
|
|
Liver disease/Hepatitis B |
2.7 |
|
|
CKD |
1.3 |
|
|
Tuberculosis |
1.3 |
|
|
Alcohol Use |
Never |
65.3 |
|
Occasional |
22.1 |
|
|
Former |
9.5 |
|
|
Daily |
2.2 |
|
|
Binge |
1.1 |
|
|
Smoking Status |
Never |
70.2 |
|
Occasional |
14.9 |
|
|
Former |
9.6 |
|
|
Heavy |
3.2 |
|
|
Daily |
2.1 |
|
|
Motion Sickness |
None |
68.4 |
|
Occasional |
14.7 |
|
|
Frequent |
14.7 |
|
|
Severe |
2.1 |
Ondansetron and dexamethasone were the most frequently prescribed. Metoclopramide and olanzapine were also used, although less frequently, while NK1 receptor antagonists were prescribed less frequently. However, full adherence was seen in 32%, partial adherence in 56%, and non-adherence in 12% of prescriptions (Table 3).
The reasons for non-adherence to antiemetic guidelines are listed in Figure 2. The most common cause for non-adherence was under-treatment (44.6%), followed by over-treatment (38.5%) and under-treatment in duration (36.1%).
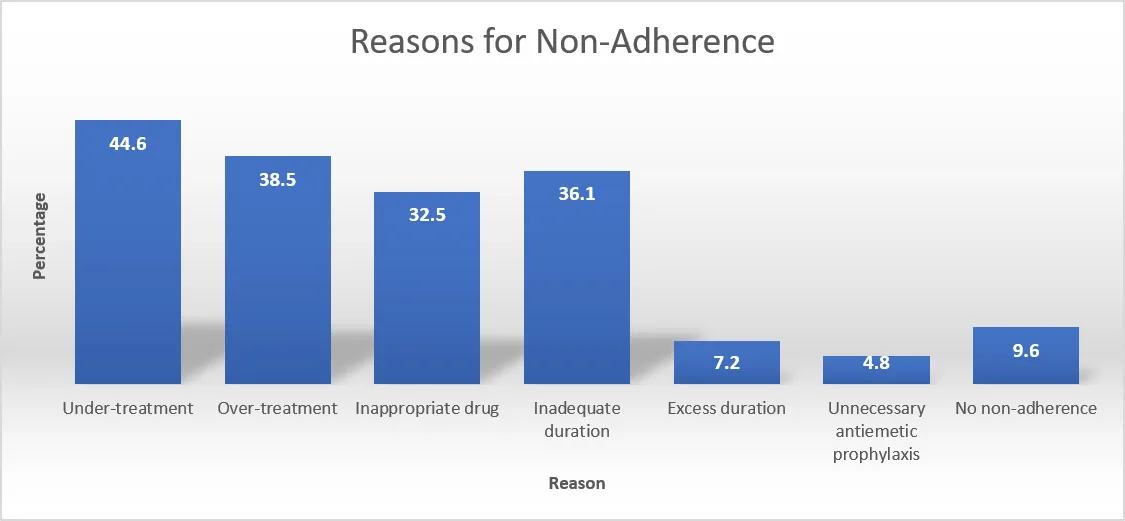
Figure 2: Reasons for Non-Adherence
Table 3. Antiemetic Utilization and Guideline Adherence
|
Variable |
Category |
Percentage (%) |
|
Antiemetic Use |
Ondansetron (5-HT3 antagonist) |
Most common |
|
Dexamethasone |
Most common |
|
|
Metoclopramide |
Less frequent |
|
|
Olanzapine |
Less frequent |
|
|
NK1 receptor antagonists |
Underutilized |
|
|
Guideline Adherence |
Fully adherent |
32 |
|
Partially adherent |
56 |
|
|
Non-adherent |
12 |
The majority of prescriptions for PPIs were recorded, constituting approximately 92% of all prescriptions. A lower percentage of patients were prescribed potassium-competitive acid blockers (P-CABs) such as Vonoprazan, which constituted approximately 3% of all prescriptions. The use of H₂ receptor antagonists, such as Famotidine, was very limited, constituting only approximately 3%. Additionally, only a small percentage of patients were prescribed mucosal protective agents such as sucralfate and combination regimens consisting of PPIs and prokinetics, constituting 2%. Most of the prescriptions which consisted of about 62.1% were overutilized. Proper utilisation of the gastric defensive drugs was identified in 35.8% of the patients and a small percentage 2.1% of underuse of the drug.
The most frequently encountered DRPs were inappropriate antiemetics (72.6%), unnecessary GPA use (65.3%), and excessive duration (55.8%). Suboptimal prophylaxis (41.1%) and drug interactions (17.9%) were also observed (Figure 3).
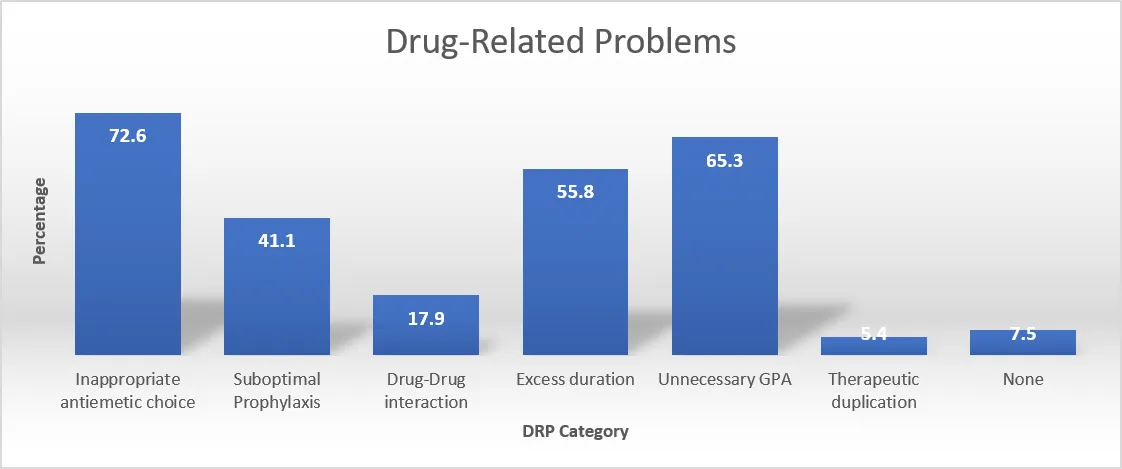
Figure 3: Distribution of Drug-Related Problems
DISCUSSION :
This study assessed the appropriateness of antiemetic and gastric protective agent use, in addition to the level of guideline adherence among oncology patients undergoing chemotherapy. The results showed a wide gap between the recommended guidelines and the actual prescribing practices, in addition to overuse of gastric protective agents.
The population studied consisted mostly of elderly individuals, which is consistent with the epidemiology of cancer. The larger proportion of females can be explained by the predominance of female breast cancer cases. This is in line with the statistics of cancer in the world, as breast cancer has been listed among the most often diagnosed malignancies[23]. The predominance of advanced-stage disease and TNM-based classifications suggests late presentation or diagnosis, which is commonly observed in developing healthcare settings.
Moderately and highly emetogenic chemotherapy regimens constituted the majority of treatments, highlighting the need for appropriate antiemetic prophylaxis. The fact that the Hesketh classification was implemented in the current study also contributes to the strength of the applied methods and makes it easier to compare it with the other risk stratification approaches according to the guidelines[24,25]. Although some proportion of the prescriptions exhibited partial or full compliance with established guidelines such as ASCO, MASCC/ESMO, and NCCN, there was a significant proportion that exhibited non-compliance. More importantly, only a small proportion of the antiemetic therapies were considered appropriate, thus showing the significant gap between the guidelines and actual practice.
Ondansetron and dexamethasone were the most frequently used, while nk1 receptor antagonists were underutilized even in highly emetogenic regimens, which resulted in the improper prescribing and non-compliance with guidelines. The results are in line with other studies wherein non-adherence to guidelines was partly due to the absence of Nk1 antagonist use[26].
Adherence to the guidelines in the present study was suboptimal, with only a small proportion of prescriptions showing good adherence and a majority showing partial adherence and a significant proportion showing poor adherence. This indicates that although clinicians may be aware of the existing antiemetic guidelines in general, application of these guidelines is poor. The most important causes of non-adherence were found to be under-treatment, over-treatment, and long duration of treatment, which may be due to inconsistent assessment of emetogenic risk and inconsistent decision-making. Inconsistent use of existing regimens may also be due to inappropriate use of drugs.
The most frequently used drugs were dexamethasone and Ondansetron, which were used together. Inasmuch as this is in line with the recommendation of certain emetogenic categories, the fact that combinations of ondansetron, metoclopramide, and olanzapine are used in inappropriate emetogenic categories creates an inclination to the use of empirical over evidence-based choices[27].
One important finding from the study was the high use of gastric protective agents, especially the use of ppis, the majority of which were not used according to the clinical indication. The misuse of PPIs as such has been ample in the oncology and general medical literature.
Drug-related problems were highly prevalent, with the main issues being the improper selection of antiemetics, the lack of necessity for the use of gastric protective agents, and the prolonged duration of treatment. These results illustrate the intricacy of drug therapy in the field of oncology and the high probability of the occurrence of irrational drug use.
Although patient-related risk factors for chemotherapy-induced nausea and vomiting were identified, these factors were not always considered in chemotherapy prescribing. This suggests that there is a lack of individualized approaches in chemotherapy.
These results reinforce the need for interventions such as education of clinicians, prescription audits, and the use of clinical pharmacists to ensure the implementation of guidelines and optimize drug use.
Limitations of the study are that the sample size was small (95 patients) and the study was conducted in a single centre. The clinical outcomes of the severity of nausea and vomiting and the quality of life of the patients are not measured in this study.
Nevertheless, the current research is useful in offering practical experience regarding the prescription of antiemetic and gastric protective agents in the clinical management of cancer patients. The current research also displays the current gaps in the applied guidelines and high prevalence of drug-related issues, particularly improper prescription and excessive use of antiemetics and gastric protective agents. This once again highlights the need for enhancing the adoption of evidence-based practices in clinical care. It could enhance the clinical management of the cancer patients by the improvement of the multidisciplinary methodology by means of clinical pharmacist involvement and the education of the prescribers and regular review of drug use.
CONCLUSION:
This study revealed that a considerable percentage of antiemetic prescriptions in adult oncology patients were not entirely in accordance with existing guidelines and that inappropriate drug use, undertreatment, and over-treatment were the most common discrepancies. The use of gastric protective agents was also found to be high, and overuse of these drugs was noted to be at a significant level, especially for PPIs. Drug-related issues were also noted to be high, reflecting the intricacies of drug therapy in the oncology setting.
This also reflects the need to improve adherence to guidelines and rational drug use practices in the management of patients. Interventions such as the involvement of clinical pharmacists and drug utilization studies may be effective in improving drug use in these settings. This will eventually improve patient safety and quality of care for these patients.
Abbreviations:
Conflict of Interest:
The authors declare no conflicts of interest.
Funding Statement:
No external funding was received for this study.
Acknowledgments:
The authors would like to sincerely thank and acknowledge the guidance and supervision of Dr. Ponni Sivaprakasam, Senior Consultant in Medical Oncology, Hemato-oncology, and BMT, Gleneagles Hospital, Chennai. The authors would like to thank Prof. Dr. Arun Ramanan V, Clinical Lead and Senior Consultant, Medical Oncology, Gleneagles Institute of Oncology, Chennai, for providing valuable support for this study as the Principal Investigator.
Ethics Approval Statement:
This study was approved by the Institutional Ethics Committee (Protocol ID: BMHR/2026/0163).
Patient Consent Statement:
For this study, patient consent was waived.
Data Availability Statement:
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES




Dipanjan Maity, Ponni Sivaprakasam, Arun Ramanan V, Satyam Arya, Evaluation of Antiemetic and Gastric Protective Agent Use and Guideline Adherence in Adult Oncology Patients: A Mixed Observational Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3775-3785. https://doi.org/10.5281/zenodo.20711066
 10.5281/zenodo.20711066
10.5281/zenodo.20711066