
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, MGSM’S Smt. Sharadchandrika Suresh Patil College of Pharmacy, Chopda, Jalgaon, Maharashtra, India 425107
Orodispersible films (ODFs) have emerged as a promising patient-centric drug delivery platform for pediatric populations due to their ability to rapidly disintegrate in the oral cavity without the need for water. The lack of age-appropriate dosage forms for children frequently necessitates dose manipulation and off-label medication use, contributing to dosing errors, reduced adherence, and administration challenges, particularly in patients with dysphagia or chronic therapeutic needs. ODFs offer several advantages over conventional pediatric formulations, including improved ease of administration, enhanced dose flexibility, reduced choking risk, and greater portability and stability. This review critically examines the current advances in pediatric ODF technology, encompassing formulation design, biopharmaceutical considerations, manufacturing technologies, and quality evaluation. Particular emphasis is placed on polymeric matrices such as pullulan, hydroxypropyl methylcellulose (HPMC), and thiolated chitosan, as well as taste-masking approaches and the incorporation of nano- and microparticulate drug delivery systems. The influence of age-dependent oral physiology, salivary composition, oro-mucosal absorption, and disintegration behavior on drug performance is discussed. Furthermore, conventional and emerging manufacturing techniques, including solvent casting, electrospinning, hot-melt extrusion, direct powder extrusion, inkjet printing, and three-dimensional (3D) printing, are evaluated with respect to scalability, personalization, and product quality. Despite significant progress, challenges related to limited drug loading capacity, moisture sensitivity, effective taste masking, excipient safety, and regulatory acceptance continue to hinder widespread clinical translation. Emerging strategies involving nanotechnology-enabled formulations, electrospun nanofibrous films, personalized printed dosage forms, and quality-by-design approaches are highlighted as potential solutions. Overall, pediatric ODFs represent a versatile and innovative dosage form with considerable potential to address unmet needs in pediatric pharmacotherapy, although further clinical and regulatory advancements are required to support their broader implementation.
Orodispersible films (ODFs) have emerged as promising age-appropriate dosage forms capable of addressing persistent challenges in pediatric pharmacotherapy. Despite significant anatomical, physiological, and developmental differences across pediatric populations, many children continue to receive off-label medicines or manipulated adult formulations. [6] 18] [19] [20]. A considerable proportion of pediatric medicines remain either unlicensed or inadequately adapted for pediatric use [24] [45]. Consequently, practices such as tablet splitting, crushing, capsule opening, and empirical dilution are frequently employed, increasing the risk of dosing errors, altered drug bioavailability, and poor therapeutic outcomes [5] [45].
Conventional pediatric formulations exhibit several limitations. Oral liquids are widely prescribed; however, they often suffer from dosing variability, chemical and microbiological instability, bulky packaging, dependence on measuring devices, and the need for preservatives or high sugar content [18] [19] [21] [22]. In addition, evidence supporting age-specific acceptability regarding formulation volume, texture, and viscosity remains limited [21]. Solid dosage forms such as tablets and capsules offer superior stability but are frequently unsuitable for younger children because of swallowing difficulties, particularly in those below 4–6 years of age [5] [18] [22]. Orodispersible tablets (ODTs) partially address these challenges by enabling water-free administration. Nevertheless, their fixed dose strengths, limited flexibility, taste-masking difficulties, and restricted suitability for modified-release delivery continue to limit their pediatric applicability [8] [18] [21]. [23] [24] [25] [26]
Recognizing these challenges, regulatory agencies and the World Health Organization increasingly advocate the development of age-appropriate and patient-centric pediatric formulations [5] [8] [18] [45]. Such formulations should ensure accurate dosing, acceptable palatability, minimal administration burden, and excipient safety while accommodating developmental and physiological variability among children[19] [21] [22]. Accordingly, swallowability, taste acceptability, dose flexibility, ease of administration, and caregiver convenience have become critical determinants of formulation success [8] [22] [45].
Within this context, ODFs represent an attractive alternative. These thin polymeric films rapidly disintegrate upon contact with saliva, enabling administration without water and reducing the risk of choking [3] [4] [13] [21] [27] [25] [28] Furthermore, ODFs may facilitate buccal or pre-gastric drug absorption, potentially improving onset of action and bioavailability for selected drugs [3] [21] [27] [28]. Unlike conventional formulations, ODFs provide greater dosing flexibility through film size adjustment and emerging digital printing technologies .Their small size, softness, and ease of administration make them particularly suitable for infants, preschool-aged children, and patients requiring individualized or long-term therapy [4] [13]. Although preliminary studies report favorable palatability and caregiver acceptance, clinical adoption remains limited, highlighting the need for further translational and clinical research [3] [27] [29]
Despite growing interest in ODF technology, current literature remains fragmented. Most available reviews focus primarily on formulation technologies or adult applications, with limited emphasis on pediatric-specific biopharmaceutics, acceptability, regulatory requirements, and real-world clinical implementation [3] [10] [21] 27] [28] [30] [32]. Similarly, broader reviews on oral and buccal drug delivery often discuss film-based systems without adequately considering the unique physiological and behavioral characteristics of pediatric patients [8] [44] [46]. This gap underscores the need for a comprehensive pediatric-focused evaluation of ODFs.
Therefore, this review critically examines the role of ODFs in pediatric drug delivery. It discusses unmet needs in pediatric pharmacotherapy and age-related factors influencing ODF performance, defines and classifies ODF systems, compares ODFs with conventional pediatric dosage forms from a patient-centric perspective, and evaluates formulation strategies, biopharmaceutical considerations, manufacturing technologies, quality assessment methods, and future development opportunities [3] [6] [21] [27] [28].
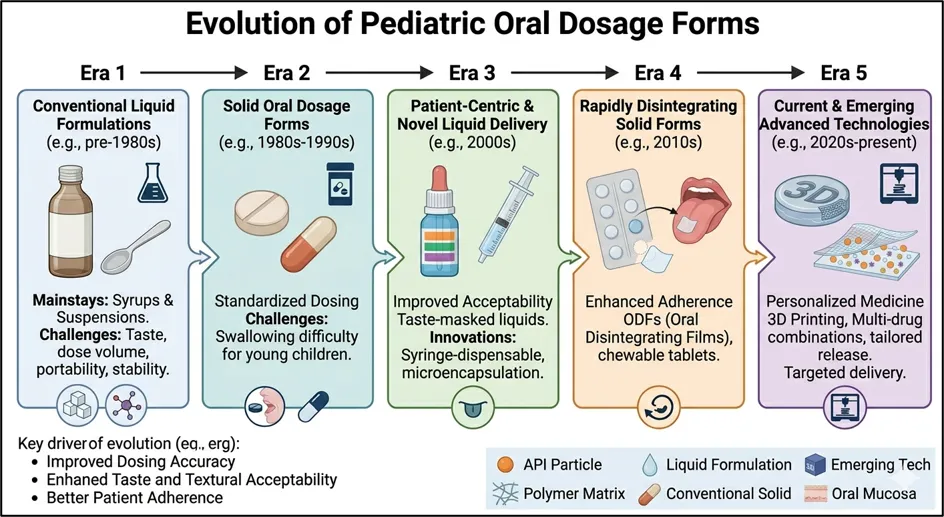
Figure 1 : Evolution of Pediatric Oral Dosage forms
Table 1 : Comparison of Orodispersible Films (ODFs) with Other Oral Dosage Forms for Pediatric Drug Delivery
|
Parameter |
Orodispersible Films (ODFs) |
Conventional Tablets |
Capsules |
Syrups/ Solution |
Orodispersible Tablets (ODTs) |
|
Administration without water |
Yes |
No |
No |
Yes |
Yes |
|
Suitability for children with dysphagia |
Excellent |
Poor |
Poor |
Good |
Very Good |
|
Risk of choking |
Very Low |
High |
High |
Very Low |
Low |
|
Dose accuracy |
High |
High |
High |
Moderate (depends on measuring device) |
High |
|
Dose flexibility |
Excellent; films can be cut or individualized |
Limited |
Limited |
Good |
Limited |
|
Disintegration time |
Very rapid (typically seconds) |
Requires swallowing and dissolution in GI tract |
Requires swallowing and dissolution in GI tract |
Immediate administration |
Rapid but generally slower than ODFs |
|
Patient acceptability/ compliance |
Excellent |
Moderate to Poor in young children |
Poor |
Good |
Very Good |
|
Portability |
Excellent; thin and lightweight |
Good |
Good |
Poor (bulky bottles) |
Good |
|
Need for swallowing ability |
No |
Yes |
Yes |
Minimal |
Minimal |
|
Taste masking potential |
Good to Excellent |
Usually not required |
Usually not required |
Variable |
Good |
|
Drug loading capacity |
Low to Moderate |
High |
High |
Moderate |
Moderate |
|
Mechanical robustness |
Flexible and less brittle |
High |
High |
Not applicable |
More brittle than ODFs |
|
Bioavailability enhancement potential |
High due to possible buccal absorption |
Conventional GI absorption |
Conventional GI absorption |
Conventional GI absorption |
Moderate |
|
Storage stability |
Sensitive to moisture; special packaging often required |
Excellent |
Excellent |
Lower than solids |
Good |
|
Manufacturing cost |
Higher |
Low |
Low |
Moderate |
Moderate |
|
Overall paediatric suitability |
Excellent |
Poor to Moderate |
Poor |
Good |
Very Good |
2. Pediatric-Specific Factors Shaping ODF Performance
2.1 Age-Dependent Physiological Differences
Pediatric anatomical and physiological characteristics strongly influence the design and performance of orodispersible films (ODFs). Infants and young children possess smaller oral cavities and reduced tongue surface area, limiting acceptable film dimensions and increasing the risk of gagging or unintended adhesion when films are oversized or excessively mucoadhesive [12] [18] [24] [31] . As oral structures develop from infancy through adolescence, film size, thickness, and placement strategies must be adapted to age-related anatomical changes [18] [24].
The pediatric oral mucosa is generally thinner and more permeable than that of adults, potentially enhancing pre-gastric drug absorption while simultaneously increasing susceptibility to excipient-related toxicity and unintended systemic exposure [8] [18] [21] [46]. Furthermore, age-related variations in mucin composition and buccal tissue characteristics may affect mucoadhesion and drug permeation, highlighting the need for careful excipient selection and safety evaluation [32].
Salivary physiology also evolves throughout childhood. Lower salivary volumes and immature secretory function in younger children may delay film hydration and disintegration, whereas adolescents exhibit oral conditions closer to those of adults [18] [31] [32]. Consequently, pediatric ODF development should integrate age-specific considerations regarding film dimensions, disintegration behavior, and permeation characteristics to ensure consistent performance and safety [18].
2.2 Salivary Environment and Its Impact on Disintegration
The salivary environment is a key determinant of ODF performance. Efficient film disintegration depends on rapid hydration, making saliva flow rate a critical factor. Reduced salivary secretion, commonly associated with dehydration, illness, or mouth breathing, can prolong disintegration and delay drug release [4] [13] [21] [31] [32]. Such variability may contribute to inconsistent in vivo performance across pediatric populations [18] [44].
Salivary pH, typically ranging from 6.2 to 6.8, influences polymer ionization, swelling, and erosion, thereby affecting both disintegration and drug release kinetics [1] [31] [32] [33] [44]. Polymer properties further modulate these effects; higher molecular-weight and more viscous polymers generally enhance mechanical strength but may slow disintegration and increase palatal adhesion [31] [32] [33]. Additionally, interactions with salivary mucins and enzymes can alter film hydration, surface morphology, and residence time, particularly in mucoadhesive systems [32]. Despite their potential importance, pediatric-specific data regarding enzyme-mediated and microbiome-related effects on ODF behavior remain limited [32] [47].
2.3 Behavioral and Administration-Related Factors
Beyond formulation attributes, successful pediatric ODF use depends on patient and caregiver behavior. Palatability, mouthfeel, and rapid disintegration are consistently identified as major determinants of acceptability and adherence [22]. Clinical studies involving children aged 6–60 months demonstrate high acceptance of ODFs by both patients and caregivers, largely due to ease of administration and swallowability [25] [31] [33]. Evidence further indicates that flexible solid dosage forms can be administered successfully even to very young infants, offering advantages in dosing accuracy and reduced spillage compared with liquid formulations [4] [13] [22].
However, favorable formulation characteristics alone do not guarantee successful administration. Incorrect placement, film folding, adherence to fingers, or inadequate caregiver familiarity may compromise dose delivery and therapeutic outcomes [25] [31]. The moisture-sensitive nature of ODFs also necessitates appropriate packaging and clear handling instructions to prevent premature hydration [8] [21]. While technologies such as dose printing and film subdivision support individualized therapy, they introduce additional risks of dosing errors and therefore require robust labeling, caregiver education, and user-friendly administration systems [13].
Critical Perspective: Although ODFs offer significant advantages for pediatric drug delivery, their performance is highly dependent on age-related oral physiology, salivary variability, and administration practices. Current evidence supports their acceptability and clinical potential, but important knowledge gaps remain regarding pediatric mucosal permeability, oral microbiome interactions, and real-world administration factors. Addressing these limitations will be essential for developing standardized, age-appropriate ODF products with predictable clinical performance.
3. Orodispersible Films: Definition, Structure, Mechanisms and Types
3.1 Definition and Structural Characteristics
Orodispersible films (ODFs) are thin, flexible polymeric dosage forms designed to disintegrate rapidly in the oral cavity without the need for water. After contact with saliva, the film forms a solution or fine dispersion, releasing the active pharmaceutical ingredient (API) for gastrointestinal absorption, local action, or transmucosal delivery [1] [11] [13] [21]. Regulatory and pharmacopoeial definitions emphasize rapid disintegration, ease of administration, adequate mechanical strength, and patient acceptability, making ODFs particularly suitable for pediatric use[1] [3] [34].
The performance of ODFs is governed by several structural attributes:
Recent developments have expanded ODF design beyond simple fast-dissolving systems. Pediatric formulations increasingly incorporate mucoadhesive polymers such as chitosan and thiolated chitosan to prolong mucosal residence and enhance local or systemic drug delivery [9] [26] [32] [48]. However, increasing structural complexity often introduces challenges related to manufacturability, reproducibility, and regulatory evaluation.
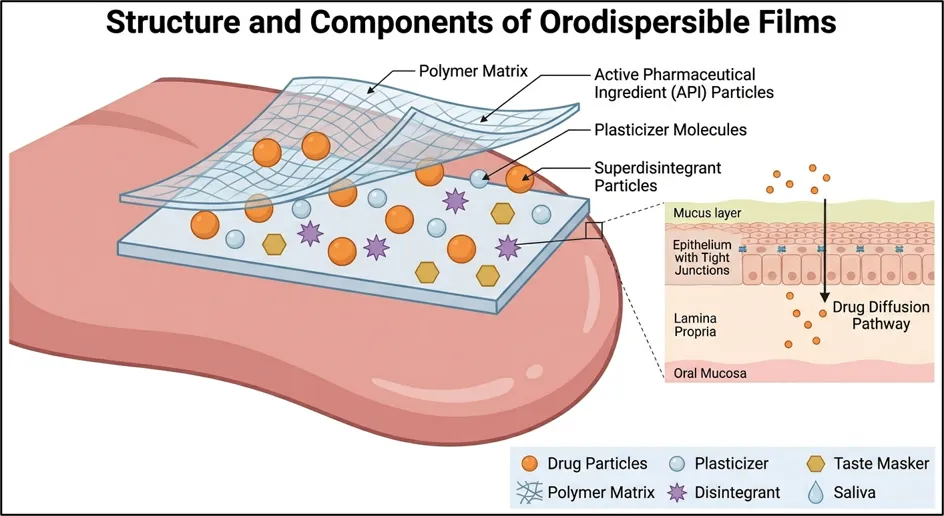
Figure 2 Structure and Components of Oroispersible Films
3.2 Mechanism of Disintegration and Drug Release
Drug release from ODFs is initiated immediately after exposure to saliva and proceeds through a sequence of interconnected processes.
Wetting
Saliva rapidly penetrates the hydrophilic matrix. The rate of wetting depends on film thickness, porosity, surface characteristics, and polymer hydrophilicity [3] [4] [21] [32] [33] [38].
Swelling
Water uptake hydrates polymer chains, causing matrix expansion and reduced intermolecular interactions. This process softens the film and prepares it for structural breakdown [3] [4] [21] [32] [34].
Disintegration and Erosion
As hydration progresses, the matrix loses cohesion and either fragments or dissolves completely. Polymer type, viscosity grade, surfactants, and disintegrants significantly influence the disintegration profile 3] [4] [21] [32] [34]..
Drug Dissolution and Release
The API is released through a combination of diffusion from the hydrated matrix and polymer erosion. Release kinetics are therefore governed by both formulation composition and matrix architecture [4] [21] [32].
For poorly water-soluble drugs, conventional diffusion mechanisms are often insufficient. Formulation strategies such as amorphous solid dispersions, nanoparticles, cyclodextrin complexes, and microparticulate systems are frequently employed to improve dissolution and bioavailability [3] [35] [38] [39] [40].
Studies on pediatric tuberculosis ODFs containing pyrazinamide demonstrated that drug release is controlled by anomalous diffusion coupled with matrix erosion, achieving complete film disintegration within approximately 35 seconds while maintaining sustained drug release for up to 60 minutes [4]. Similarly, nanoparticle-loaded ODFs function as carrier platforms, releasing colloidal particles after film disintegration, whereas microparticle-based systems can separate rapid oral disintegration from prolonged gastrointestinal drug release [5] [8].Critically, film disintegration does not necessarily predict drug-release kinetics. Advanced multilayer and particulate-containing systems increasingly decouple these processes, enabling more sophisticated therapeutic profiles while preserving patient-friendly administration [8] [40].
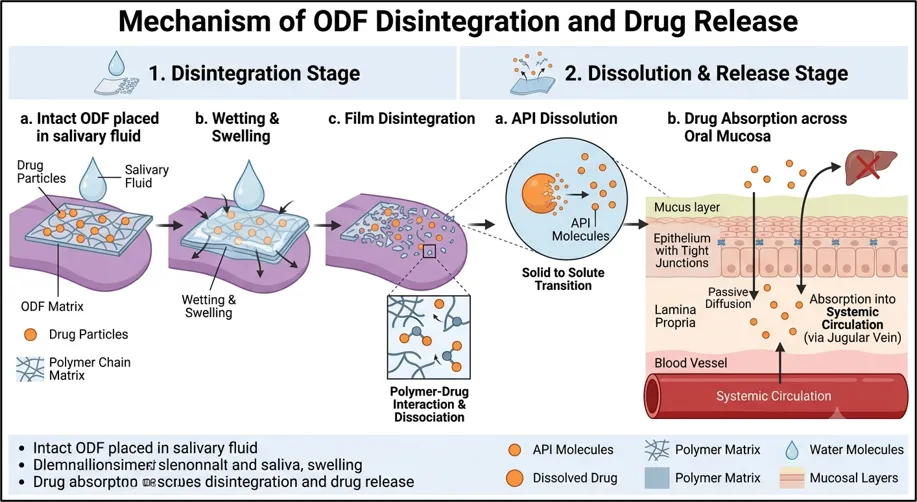
Figure 3 Mechanism of Disintegration and Drug Release
3.3 Classification of Orodispersible Films
A. Based on Drug Loading
Low-Dose Films
These films are intended for potent drugs requiring only microgram-to-low milligram doses. Uniform drug distribution is critical because small variations can significantly affect dose accuracy [4] [11] [13] [35][41].
Medium-Dose Films
Dose delivery is achieved through larger film dimensions or administration of multiple film units. These systems provide greater dosing flexibility but may affect convenience and patient acceptance [4] [8].
High-Load Films
High-load ODFs can accommodate approximately 30–100 mg of API through increased drug content or incorporation of particulate systems. However, higher drug loading often increases thickness, reduces flexibility, and complicates manufacturing, making this category one of the major formulation challenges in pediatric ODF development [8] [21] [35] [36] [40] [42] .
B. Based on Polymer Composition and Structure
Monolayer Films
Monolayer systems contain all formulation components within a single matrix and remain the most widely used ODF design because of their simplicity and ease of manufacture [3] [33] [38].
Fast-Disintegrating Hydrophilic Films
These formulations are composed primarily of hydrophilic polymers such as cellulose derivatives, HPC, and PVA. Their primary objective is rapid dispersion and immediate drug release following swallowing [3] [4] [13] [31] [32] [35] [36].
Mucoadhesive Films
Mucoadhesive systems incorporate polymers such as chitosan or thiolated derivatives to prolong residence time and facilitate localized or transmucosal drug absorption [9] [26] [32] [48].
Multilayer Films
Bilayer and trilayer architectures provide functional separation of components and can improve taste masking, drug stability, permeability control, and unidirectional drug delivery [10] [33] [38].
Examples include:
Modified-Release Matrices
Although ODFs are traditionally associated with immediate release, incorporation of hydrophobic polymers, barrier layers, coated particles, or multiparticulate systems can produce delayed or sustained-release profiles [3] [8] [40].
C. Based on Absorption Pathway
Gastrointestinal-Oriented ODFs
In these systems, the drug is primarily swallowed after film disintegration and absorbed through the gastrointestinal tract. The main advantage is improved convenience and potentially faster onset due to pre-dissolution in saliva [4] [5] [13] [11] [35].
Oromucosal ODFs
These films are designed for buccal or sublingual absorption, enabling partial or complete avoidance of first-pass metabolism. Mucoadhesive layers and permeability-modifying components are commonly incorporated to improve drug uptake and therapeutic efficiency [3] [9] [10] [26] [32] [38] [48].
Hybrid Systems
Hybrid ODFs combine rapid oral disintegration with prolonged drug release. Typically, they incorporate coated microparticles, pellets, or sustained-release carriers that continue releasing drug after swallowing. Such systems integrate the administration advantages of ODFs with extended systemic exposure [8] [40].
Critical Perspective
Current ODF technology has evolved from simple fast-dissolving films to multifunctional delivery platforms capable of immediate, mucoadhesive, and controlled-release drug delivery. Nevertheless, increasing formulation complexity often introduces trade-offs between drug loading, mechanical properties, disintegration rate, and manufacturability[8] [35] [40] . While multilayer and hybrid systems expand therapeutic possibilities, pediatric-specific evidence supporting their long-term safety, clinical performance, and large-scale production remains limited. Future development should therefore focus on balancing formulation sophistication with robustness, scalability, and age-appropriate design requirements to maximize clinical translation in pediatric medicine[8] [13] [21].
4. Advantages and Limitations of Orodispersible Films for Pediatric Use
4.1 Advantages from a Formulation and Biopharmaceutical Perspective
Rapid Disintegration and Ease of Administration
One of the principal advantages of ODFs is their rapid disintegration in the oral cavity, typically occurring within seconds to less than one minute. Several pediatric formulations have achieved disintegration times well below the pharmacopoeial limit of 180 seconds, with some disintegrating in under 40 seconds. This enables administration without water and minimizes swallowing difficulties, making ODFs particularly suitable for infants and children with poor cooperation or dysphagia [4] [13] [18] . Compared with conventional tablets and capsules, ODFs offer a more patient-friendly dosage form that can improve treatment adherence.
Accurate and Flexible Dosing
ODFs provide a high degree of dose precision and adaptability. Drug loading can be controlled through film size, drug concentration, or printing technologies, facilitating individualized dosing for pediatric patients [4] [13] [21]. Studies on printed warfarin ODFs demonstrated accurate dose delivery across a range of 0.1–2 mg with superior content uniformity compared with conventional powder formulations [13]. Such flexibility is particularly valuable for weight-based dosing and drugs with narrow therapeutic indices.
Potential for Rapid Absorption and Improved Bioavailability
ODFs can support drug absorption through the highly vascularized oral mucosa, offering opportunities for faster therapeutic onset and partial avoidance of first-pass metabolism [46] [26] [9] [48]. Mucoadhesive and buccal film systems further enhance mucosal residence time and drug permeation, enabling both local and systemic delivery [9] [26] [46] [48]. These attributes have attracted interest in pediatric applications requiring rapid therapeutic action, including tuberculosis and pain management therapies [4] [8] [9]
Improved Stability and Distribution
As solid dosage forms, ODFs generally exhibit greater physicochemical stability than liquid formulations and often eliminate the need for preservatives . Their low weight, compact size, and reduced storage requirements simplify transportation and distribution, particularly in resource-limited settings [4] [5] [18] [4]. Available studies also indicate acceptable short-term stability for both solvent-cast and printed films under controlled conditions [4] [13].
Enhanced Palatability
Taste masking remains a critical factor in pediatric medicine, and ODFs provide opportunities for incorporating advanced taste-masking technologies. Approaches such as cyclodextrin complexation, pH-responsive polymers, nanoparticle encapsulation, and multiparticulate systems have demonstrated effective masking of bitter drugs while maintaining drug release and bioavailability [4] [5] [45]. These strategies can substantially improve patient acceptance and adherence, particularly for chronically administered medications.
4.2 Formulation and Developmental Limitations
Limited Drug-Loading Capacity
Despite their advantages, ODFs are inherently constrained by limited drug-loading capacity. Increasing drug content often results in thicker films, reduced flexibility, impaired mechanical strength, and slower disintegration [8] [13] [21]. Consequently, high-dose therapies may require multiple films per administration, potentially reducing convenience and patient acceptance [4]. Achieving high drug loading while preserving desirable film characteristics remains a major formulation challenge.
Taste-Masking and Mouthfeel Challenges
Because ODFs disintegrate directly on the tongue, unpleasant taste and poor mouthfeel are immediately perceived by the patient. Bitter APIs and particulate-based formulations may cause grittiness or residual sensations that negatively affect acceptability [5] [18] [22]. Although advanced taste-masking approaches are effective, they often increase formulation complexity, manufacturing costs, and development time [4] [5] [8] [48].
Moisture Sensitivity and Stability Concerns
Most ODFs are composed of hydrophilic polymers that readily absorb moisture from the environment. Excessive humidity can alter mechanical properties, promote sticking, accelerate degradation, and reduce product performance [8] [21] [22]. As a result, ODFs generally require protective moisture-barrier packaging and rigorous stability assessment, particularly when formulated with amorphous drugs or nanostructured delivery systems.
Challenges in Controlled Drug Release
The rapid-disintegration nature of ODFs inherently favors immediate drug release. Developing sustained- or controlled-release systems within this platform remains technically challenging [8] [21]. Recent approaches involving mucoadhesive matrices, multilayer structures, coated microparticles, and thiomer-based systems have shown promise, but these designs require more sophisticated materials and manufacturing processes [8] [9]. Consequently, balancing rapid administration with prolonged therapeutic action remains a significant developmental hurdle.
Excipient Safety and Regulatory Considerations
The use of specialized excipients, including permeation enhancers, novel mucoadhesive polymers, and certain plasticizers, raises safety concerns in pediatric populations, particularly in neonates and infants [8] [22]. Many of these materials lack extensive pediatric safety data, leading to increased regulatory scrutiny and more stringent risk–benefit assessments [8] [21]. This limitation may slow clinical translation despite promising formulation performance.
Critical Perspective
ODFs address several longstanding challenges in pediatric drug delivery by combining ease of administration, dose flexibility, improved palatability, and the potential for enhanced bioavailability[13] [18] [21]. However, these benefits are offset by formulation constraints, particularly limited drug loading, moisture sensitivity, and the complexity of taste masking and controlled-release design [8] [21]. Furthermore, the limited pediatric safety data available for several functional excipients remains a critical barrier to wider regulatory acceptance [8] [22]. Future research should focus on optimizing high-load formulations, establishing pediatric-specific excipient safety profiles, and developing scalable manufacturing approaches that maintain the patient-centered advantages of ODF technology.
5. Biopharmaceutical and Pharmacokinetic Considerations
5.1 Oral Mucosal Permeability and Drug Absorption
The oral mucosa plays a critical role in determining the absorption profile of pediatric ODFs. Compared with adults, pediatric oral mucosa is generally thinner and more permeable, which may enhance drug transport across the epithelium but also increase susceptibility to excipient-related toxicity [1] [4] [8] [10] [49] [52]. This dual effect highlights the need to balance absorption enhancement with safety considerations during formulation development.
Mucoadhesive ODFs based on cellulose derivatives, chitosan, and thiolated polymers can prolong mucosal residence time and improve drug permeation across buccal tissues [9] [16] [1] [8] [32] [49]Enhanced permeation has been demonstrated for drugs such as lidocaine, suggesting potential for improved local or systemic delivery [9] [16].
The extent of absorption depends on both formulation design and therapeutic objective. For example, clobetasol-loaded films achieve high local tissue retention with minimal systemic exposure, making them suitable for localized therapy [16] [53]. In contrast, bilayered and unidirectional films can facilitate transmucosal delivery of systemic drugs by directing drug release toward the mucosal surface while minimizing drug loss into saliva[48] [53].
Despite these advantages, the contribution of buccal absorption to overall drug exposure remains highly drug-dependent and is not yet fully characterized in pediatric populations [49] [52].
5.2 Impact of Rapid Drug Release on Pharmacokinetics
A defining feature of ODFs is their rapid disintegration and drug release. Electrospun and solvent-cast pediatric films have demonstrated disintegration times ranging from 1 to 35 seconds, with complete drug release often occurring within one hour[2] [4] [7] [11] [51] [52].
Rapid dissolution may accelerate drug absorption, potentially resulting in higher peak plasma concentrations (Cmax) and shorter times to reach maximum concentration (Tmax) compared with conventional solid dosage forms [2] [4] [7] [11] [51] [52]. This effect has been observed in micelle-loaded ebastine ODFs, which produced higher Cmax values and reduced Tmax relative to oral suspensions [52].
However, rapid release may also increase the risk of dose dumping, particularly for drugs with a narrow therapeutic window[2] [4]. Although clinical evidence remains limited, this concern highlights the importance of carefully controlling release kinetics during formulation development.
To address this challenge, advanced ODF platforms have incorporated sustained-release microparticles within rapidly disintegrating films. Topiramate sustained-release ODFs successfully separated film disintegration from drug-release kinetics and achieved bioequivalence to extended-release capsules while maintaining a smoother pharmacokinetic profile [8] [2]. These findings demonstrate that rapid oral disintegration and controlled systemic delivery are not mutually exclusive.
5.3 Avoidance of First-Pass Metabolism
One of the most frequently cited advantages of oromucosal drug delivery is the potential to bypass hepatic first-pass metabolism. Drugs absorbed through the buccal or sublingual mucosa may enter systemic circulation directly, thereby improving bioavailability and reducing metabolic losses [33] [49] [52] [54] [48].
Mucoadhesive and thiomer-based ODFs have demonstrated the ability to modulate drug exposure through prolonged contact with the oral mucosa, supporting both local and systemic therapeutic applications [9] [16]. Such systems are particularly attractive for drugs with extensive first-pass metabolism or poor oral bioavailability [49] [54].
Nevertheless, the clinical significance of this advantage should not be overstated. For many pediatric ODF formulations, including those containing anti-tubercular agents, warfarin, and sildenafil, the predominant absorption pathway remains gastrointestinal following swallowing of the dissolved drug [4] [2] [7] [51] [52]. Consequently, the extent of first-pass avoidance varies substantially between formulations and remains insufficiently quantified in pediatric patients [4] [49] [52].
5.4 Challenges in Establishing In Vitro–In Vivo Correlation
Establishing reliable in vitro–in vivo correlation (IVIVC) for pediatric ODFs remains challenging. Unlike conventional oral dosage forms, ODF performance is influenced by age-dependent physiological factors, including saliva volume, saliva flow rate, oral movements, and swallowing behavior[2] [4] [10] [11] [49] [55].
Current in vitro disintegration and dissolution methods often fail to replicate the dynamic environment of the pediatric oral cavity, limiting their predictive value [11] [33]. As a result, laboratory performance may not accurately reflect in vivo drug absorption.
Successful Level A IVIVC has been reported for topiramate sustained-release ODFs because drug release from embedded microparticles, rather than film disintegration, governed overall absorption kinetics [2] [8]. In contrast, immediate-release ODFs frequently exhibit more complex release mechanisms involving diffusion, erosion, rapid dissolution, and variable contributions from buccal and gastrointestinal absorption[2] [4] [6] [11] [51].
Furthermore, emerging technologies such as electrospun nanofiber films introduce additional formulation variables that complicate prediction of in vivo behavior[11] [51]. Consequently, the development of physiologically relevant pediatric testing models remains a key research priority.
Critical Perspective
The biopharmaceutical advantages of pediatric ODFs stem from rapid disintegration, potential transmucosal absorption, and the possibility of avoiding first-pass metabolism [33] [49] [52]. However, these benefits are highly formulation- and drug-dependent rather than intrinsic to all ODF systems. While mucoadhesive and multilayer platforms can enhance mucosal uptake, most currently available pediatric ODFs still rely predominantly on gastrointestinal absorption after swallowing [4] [2] [7] [52].
A major limitation remains the lack of robust pediatric pharmacokinetic and IVIVC data. Age-related differences in oral physiology, combined with the complexity of drug release and absorption mechanisms, reduce the predictive value of conventional in vitro tests [4] [10] [49] [55]. Future research should therefore focus on developing pediatric-specific biopharmaceutical models and clinical pharmacokinetic studies to support rational formulation design and regulatory acceptance of ODF-based therapies [4] [2] [55].
6. Formulation Design of Pediatric Orodispersible Films
6.1 Film-Forming Polymers
Film-forming polymers constitute the structural backbone of ODFs and largely determine disintegration, mechanical strength, mucoadhesion, and printability.
Natural polymers
Semi-synthetic polymers
Synthetic polymers
Selection criteria
For pediatric products, polymers should ideally possess GRAS status, low residual-solvent risk, adequate strength at minimal thickness, non-toxic degradation products, and low allergenic potential [1] [6] [11] [15] [17] [32] [33].
Critically, polymer selection represents a trade-off: highly hydrophilic polymers improve disintegration but may increase moisture sensitivity, whereas stronger polymers may slow film breakup and reduce patient comfort.
6.2 Plasticizers and Mechanical Property Optimization
Plasticizers such as glycerol, sorbitol, polyethylene glycols, and triacetin reduce brittleness and improve flexibility, enabling thin films to withstand handling and packaging stresses [1] [33] [17] [49] [57].
In pediatric films manufactured by direct powder extrusion (DPE) printing, plasticizer type markedly affects tensile strength, elongation, and mucoadhesive behavior, particularly in thiomer-containing systems [1] [9].
However, excessive plasticization can be detrimental. Over-plasticized films become tacky, absorb more moisture, and exhibit poorer handling and storage stability [1] [3] [17] [33] [49]. Thus, mechanical optimization requires balancing flexibility with dimensional and physicochemical stability.
6.3 Sweeteners, Flavors, and Saliva-Stimulating Agents
Palatability is a major determinant of pediatric adherence.
Common excipients include
Organic acids such as citric and malic acid can stimulate salivation, thereby accelerating wetting and disintegration.[12] [33] [49].
For pediatric safety, ethanol-free flavor systems, controlled sweetener levels, and avoidance of high-fructose syrups are generally preferred.[10] [33] [51].
Nevertheless, optimizing sweetness remains challenging because excessive flavoring may alter film texture, stability, or dissolution behavior.
6.4 Taste-Masking Strategies
Particle coating
Embedding coated microparticles or pellets within ODFs can reduce direct drug contact with taste buds. Dual-coated sustained-release microparticles have successfully masked the bitterness of topiramate while simultaneously controlling drug release[2] [8]. Similar approaches using coated pellets or nanocrystals have been explored for other bitter APIs [11] [33].
Complexation
Cyclodextrin inclusion complexes, including HP-β-CD systems, improve both solubility and taste for drugs such as clobetasol, donepezil, and hydrocortisone, while supporting buccal or mucoadhesive delivery [4] [6] [8] [16] [58] [56].
Polymeric and resin-based approaches
pH-sensitive cationic polymers such as Eudragit E can suppress drug dissolution at salivary pH, thereby masking bitterness while allowing rapid release after swallowing [4] [33] [6]. Ion-exchange resin systems are conceptually suitable for ODFs but remain less extensively studied in pediatric formulations.
Combining microencapsulation, mucoadhesive matrices, and sweeteners enables multilayer taste-masking strategies tailored to pediatric sensory preferences [1] [6] [9] [33].
Critical Perspective
Current evidence indicates that successful pediatric ODF design depends on integrating polymer science, mechanical engineering, and sensory optimization rather than optimizing any single parameter. Highly hydrophilic films may disintegrate rapidly but suffer from poor moisture stability; stronger matrices improve handling but may compromise disintegration and comfort [1] [32] [33]. Similarly, advanced taste-masking technologies can substantially improve acceptability, yet they often increase formulation complexity, manufacturing cost, and regulatory burden [2] [6] [8].
Therefore, the most clinically relevant pediatric ODFs are likely to be those that achieve a balanced profile of rapid disintegration, acceptable mouthfeel, adequate mechanical strength, scalable manufacturing, and excipient safety, rather than maximizing a single formulation attribute [1] [8] [33].
Table 2: Comparative Evaluation of Film-Forming Polymers Used in Pediatric Orodispersible Films (ODFs)
|
Polymer |
Type |
Advantage |
Limitation |
Suitability |
Citation |
|
HPMC |
Semi-synthetic |
Strong films, good mechanical strength |
Slower disintegration at high viscosity |
High |
[30][32][59] |
|
HPC |
Semi-synthetic |
Flexible films, rapid hydration |
Lower strength than HPMC |
High |
[30][32] |
|
Pullulan |
Natural |
Ultra-fast dissolution, tasteless |
Moisture sensitive |
Very High |
[7][30][33] |
|
PVA |
Synthetic |
Excellent flexibility and strength |
Synthetic polymer |
Moderate–High |
[30][49] |
|
PVP |
Synthetic |
Enhances drug solubility and drug dispersion |
Hygroscopic, brittle alone |
Moderate |
[30][49] |
|
Sodium Alginate |
Natural |
Biocompatible, rapid disintegration |
Weak mechanical properties |
High |
[33][44] |
|
Maltodextrin |
Natural |
Fast dissolving, pleasant mouthfeel |
Lower film strength |
High |
[10] [36] |
|
Gelatin |
Natural protein |
Good mouthfeel and flexibility |
Animal origin, moisture sensitive |
Moderate–High |
[30][59] |
|
Pectin |
Natural |
Biodegradable, safe |
Poor water resistance |
High |
[33][44] |
|
CMC |
Semi-synthetic |
Rapid hydration and swelling |
Hygroscopic |
High |
[30][32] |
|
Starch |
Natural |
Low cost, biodegradable |
Brittle films |
Moderate |
[33][59] |
|
Chitosan |
Natural |
Mucoadhesive, antimicrobial |
Bitter taste, limited solubility |
Moderate–High |
[44][46] |
7. Safety Considerations of Excipients in Pediatric Orodispersible Films
The safety of excipients is a critical aspect of pediatric ODF development because children are not merely “small adults.” Age-dependent differences in metabolism, organ maturation, body composition, and mucosal permeability can significantly alter excipient exposure and toxicity profiles. Consequently, excipients considered safe in adults may not necessarily be appropriate for pediatric populations, particularly neonates and infants [6] [10] [12] [33]. Given the relatively high excipient-to-drug ratio often required in ODF formulations, excipient selection must be supported by robust toxicological and regulatory evidence.
7.1 Excipients of Regulatory Concern in Pediatrics
Regulatory agencies have identified several excipients that require particular caution in pediatric formulations due to their potential toxicity or age-related safety concerns. These include ethanol, propylene glycol, benzyl alcohol, parabens, certain surfactants, and excessive amounts of sweetening agents [6] [10] [12] [33] [59]. Adverse effects associated with these excipients may be amplified in younger children because of immature metabolic pathways and reduced detoxification capacity [10] [12].
For pediatric ODFs, additional concerns arise from the route of administration. Unlike conventional oral dosage forms, ODFs remain in direct contact with the oral mucosa before swallowing, increasing the potential for local tissue exposure and absorption of excipients [9] [12] [16] [32] [49]. This issue is particularly relevant for permeation-enhancing excipients such as thiomers, chitosan derivatives, and surfactants designed to modify epithelial barrier function [9] [12] [16] [32] [49].
While these excipients may improve drug absorption and therapeutic efficacy, they may also increase unintended systemic exposure and alter mucosal integrity, especially in children whose oral mucosa is generally more permeable than that of adults [12] [32] [49]. Therefore, the inclusion of permeability-modifying agents should be justified by clear therapeutic benefits and supported by comprehensive safety evaluation.
A key limitation of the current literature is that many novel excipients are assessed primarily for their pharmaceutical performance rather than their long-term pediatric safety. As a result, safety data often lag behind formulation innovation.
7.2 GRAS Status and Acceptable Daily Intake
Most excipients commonly used in ODF formulations possess established safety records and are generally recognized as safe (GRAS). These include widely used film-forming polymers such as pullulan, cellulose ethers, and polyvinyl alcohol, as well as plasticizers including glycerol and sorbitol [1] [7] [12] [17] [32] [33]. Polyol-based sweeteners also have extensive histories of use in pharmaceutical and food products [12] [17] [33].
However, GRAS designation alone does not guarantee safety in all pediatric settings. Risk assessment must consider age-specific exposure levels, frequency of administration, duration of therapy, and cumulative intake from multiple sources [10] [12] [17] [33]. This consideration is particularly important for pediatric ODFs because the amount of excipient may substantially exceed the quantity of API, especially in formulations containing highly potent drugs [10] [33].
Acceptable daily intake (ADI) calculations should therefore be performed on a body-weight basis and should account for worst-case scenarios, including repeated daily administration and chronic treatment regimens [10] [12] [17] [33]. Failure to consider cumulative excipient exposure may result in inadvertent exceedance of recommended safety limits despite compliance at the individual-dose level.
Furthermore, pediatric-specific ADI data are unavailable for several emerging excipients used in advanced ODF formulations. This gap complicates risk assessment and often necessitates conservative formulation strategies during product development.
7.3 Long-Term and Cumulative Exposure Risks
The importance of excipient safety extends beyond acute toxicity. Many pediatric conditions, including epilepsy, allergic disorders, and chronic inflammatory diseases, require prolonged treatment, increasing the relevance of cumulative excipient exposure[1] [9] [8] [16] [59].
Repeated administration of ODFs may lead to sustained exposure to sweeteners, flavoring agents, plasticizers, mucoadhesive polymers, and other functional excipients [1] [9] [8] [16] [59]. Although these substances are generally considered safe at therapeutic levels, the consequences of chronic exposure in developing pediatric populations remain incompletely understood.
Particular attention has focused on next-generation mucoadhesive materials, including thiolated and S-protected thiolated chitosan derivatives. These polymers have demonstrated promising performance in enhancing mucosal adhesion and drug permeation, but long-term pediatric safety data remain limited[1] [9] [6] [16] [32] [49] [59]. Potential concerns include chronic mucosal irritation, alterations in epithelial barrier function, hypersensitivity reactions, and cumulative local exposure effects.
The absence of extensive clinical safety data for these novel materials highlights a significant translational challenge. While short-term studies often demonstrate acceptable tolerability, evidence regarding long-term use, repeated exposure, and developmental safety remains insufficient [9] [16] [32] [49] [59].
Consequently, comprehensive toxicological assessment should extend beyond conventional acute toxicity studies and include evaluations of mucosal compatibility, allergenicity, chronic exposure, and developmental safety. Post-marketing surveillance will also play a critical role in identifying rare or delayed adverse effects that may not be detected during pre-approval studies[1] [6] [59].
Critical Perspective
Excipient safety represents one of the most important yet underexplored aspects of pediatric ODF development. Although most conventional film-forming polymers, plasticizers, and sweeteners possess established safety profiles, emerging functional excipients designed to enhance mucoadhesion, permeability, and drug delivery introduce new toxicological uncertainties [1] [9] [33]. The increased permeability of pediatric oral mucosa further amplifies concerns regarding systemic exposure and local tissue effects[32] [49].
Current regulatory frameworks emphasize excipient justification and risk assessment; however, pediatric-specific safety data remain limited for many innovative ODF components [10] [12] [59]. Consequently, formulation development should adopt a precautionary approach, prioritizing excipients with established pediatric use whenever possible and rigorously evaluating novel materials before clinical implementation.
Future research should focus on generating long-term toxicological data, establishing pediatric-specific exposure thresholds, and developing standardized methodologies for assessing mucosal safety. Such efforts are essential to ensure that advances in ODF technology are accompanied by an equally robust understanding of excipient safety, thereby supporting the development of effective and clinically acceptable pediatric medicines [9] [16] [49] [59].
8. Drug Candidates Suitable for Pediatric Orodispersible Films
8.1 Physicochemical and Dose-Related Selection CriteriaIdeal candidates have low dose (<20 mg per unit), sufficient solid-state stability at room temperature and buccal pH, acceptable solubility/permeability, and significant benefit from improved adherence, rapid onset, or avoidance of first-pass metabolism[2] [4] [7] [6] [11] [33] [51] . BCS I drugs are most common, but nanoparticle and microparticle technologies extend applicability to BCS II/IV [4] [6] [11] [33].
8.2 Therapeutic Classes Investigated
Table 3 : Class of Drugs and Examples
|
Class |
Examples & Pediatric Rationale |
Citations |
|
Antipyretics/ Analgesics |
Lidocaine local anesthetic ODFs; paracetamol/NSAID films |
[1] [9] [10] [12] [33] [49] |
|
Antihistamines |
Ebastine micelle-loaded ODFs with improved bioavailability |
[1] [3] [33] [52] |
|
Antiepileptics |
Topiramate sustained-release SRODFs with human bioequivalence to Qudexy XR |
[2] [8] |
|
Antiemetics |
Ondansetron ODF for CINV/PONV |
[3] [10] [49] [53] |
|
Anti-TB |
Pyrazinamide and isoniazid ODFs for improved adherence |
[2] [4] |
|
Antiretrovirals |
LPV/RTV nanoparticle ODF platforms improving taste and bioavailability |
[6] |
|
Cardiovascular/ Anticoagulants |
Warfarin printed ODFs enabling precise micro-dosing |
[13] [17] [51] |
|
Steroids/Others |
Clobetasol/hydrocortisone buccal films; sildenafil ODFs |
[7] [8] [16] [56] |
8.3 Limitations for High-Dose and Poorly Stable Drugs
The limited mass (<200 mg) and area of pediatric ODFs restrict feasible doses; multiple films or highly potent APIs are required for TB and other indications [2] [3] [4] [15] [33] [55]. APIs unstable at neutral buccal pH, moisture-sensitive drugs, or those causing mucosal irritation are poor candidates [4] [3] [6] [15] [33] [49] [55]. Complex nanoparticle or SR microparticle approaches can expand the space but add cost and regulatory complexity [8] [4] [33] [6] .
9. Manufacturing Technologies for Orodispersible Films
The selection of an appropriate manufacturing technology is a critical determinant of ODF quality, scalability, dose precision, and clinical performance. Conventional methods such as solvent casting remain dominant in commercial production, whereas emerging technologies including electrospinning and pharmaceutical printing are expanding opportunities for personalized pediatric therapy. Each platform offers distinct advantages and limitations regarding drug loading, process efficiency, stability, and regulatory feasibility.
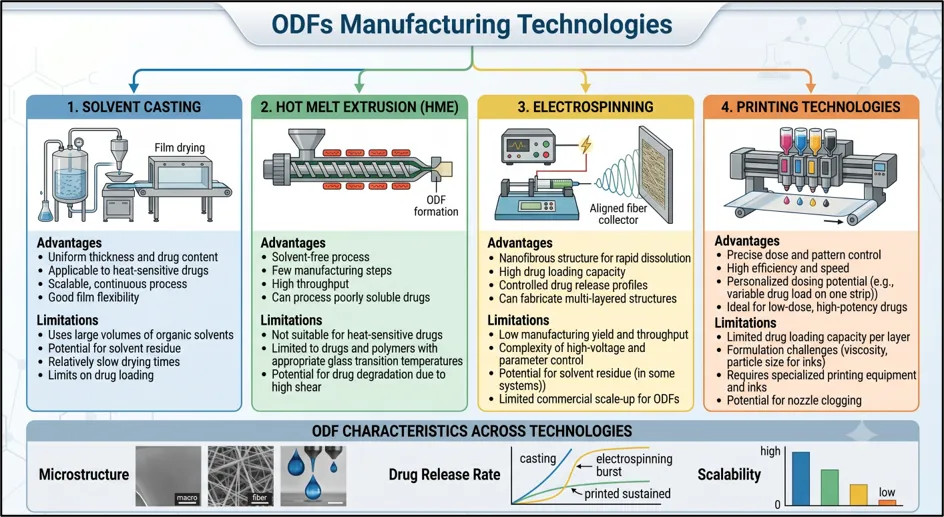
Figure 5 : ODF’s Manufacturing Technologies
9.1 Solvent Casting
Solvent casting is the most established and widely adopted manufacturing method for ODF production. In this process, the API and excipients are dissolved or dispersed in a polymeric solution, cast onto a substrate, dried, and subsequently cut into individual dosage units[3] [14] [33] [50].
The technique offers excellent film uniformity, ease of processing, and industrial scalability. However, product quality is highly dependent on formulation viscosity and drying conditions. Common challenges include residual solvent retention, air entrapment, polymorphic transformations, and content non-uniformity, particularly during large-scale manufacturing [3] [33] [50]. Consequently, stringent process control is required to ensure batch-to-batch consistency.
9.2 Hot Melt Extrusion (HME)
Hot melt extrusion is a solvent-free and continuous manufacturing process in which drug and excipients are blended under heat and pressure to form films [3] [14] [33] [63].
A major advantage of HME is its suitability for preparing amorphous solid dispersions (ASDs), thereby improving the dissolution of poorly water-soluble drugs [33] [63]. Comparative studies indicate that HME-produced films can achieve disintegration and dissolution profiles comparable to solvent-cast films while demonstrating good long-term stability when plasticizer distribution is properly optimized [63].
Despite these advantages, the high processing temperatures may cause degradation of thermolabile APIs and excipients, limiting the applicability of HME for temperature-sensitive pediatric formulations [3] [14] [33].
9.3 Electrospinning
Electrospinning produces nanofibrous ODFs characterized by extremely high surface area and porous structures, resulting in exceptionally rapid hydration and disintegration [7] [50]. Disintegration times as low as one second have been reported, making this technology attractive for pediatric applications requiring immediate drug release[7] [50].
A notable example is the development of pullulan–sildenafil ODFs for pediatric pulmonary hypertension using an aqueous electrospinning process, thereby avoiding organic solvents [7].
However, broader industrial adoption remains limited. Many electrospinning systems require organic solvents, and the resulting amorphous nanofibers may exhibit storage instability, moisture sensitivity, and recrystallization during long-term storage [3] [7] [50]. These challenges continue to restrict large-scale commercialization.
9.4 Printing Technologies for Personalized Pediatric Dosing
Inkjet and Two-Dimensional (2D) Printing
Inkjet printing enables deposition of precise quantities of drug-containing ink onto blank film substrates, making it particularly suitable for individualized dosing [13] [15]. Applications include pediatric warfarin and metoprolol ODFs, where flexible dose strengths can be produced without altering film dimensions [13] [15].
Although excellent content uniformity can be achieved, dose accuracy may be influenced by nozzle wear, printing parameters, and interactions between the ink and substrate [15] [62].
Three-Dimensional (3D) Printing and Direct Powder Extrusion (DPE)
3D printing and DPE technologies enable direct fabrication of drug-loaded ODFs with customized geometries, multilayer architectures, and tailored release characteristics [9] [11] [9] [16] [62].
These approaches offer greater design flexibility than conventional manufacturing methods and can improve content uniformity and mechanical performance through controlled deposition and in-process drying [9] [16] [62]. Pediatric applications include personalized warfarin, clobetasol, and lidocaine ODFs with adjustable doses, residence times, and release profiles [9] [13] [16].
Despite their potential, regulatory standardization, production speed, and large-scale implementation remain significant challenges.
Micro-Dispensing
Micro-dispensing employs drop-on-demand deposition of viscous formulations to produce substrate-free films [62]. The technology provides a linear relationship between deposited area and delivered dose, supporting accurate dose personalization.
Studies have shown that micro-dispensed films exhibit disintegration characteristics comparable to conventionally cast films while offering improved flexibility in dose adjustment [62]. However, industrial experience with this technology remains limited.
Critical Perspective
Manufacturing technologies for ODFs are evolving from conventional mass-production approaches toward digitally controlled, patient-centric platforms. Solvent casting remains the industrial benchmark due to its maturity and scalability, whereas HME offers solvent-free continuous processing and improved performance for poorly soluble drugs [33] [50] [63]. Electrospinning provides unmatched disintegration rates but faces stability and scale-up challenges [7] [50].
Among emerging technologies, pharmaceutical printing represents the most promising approach for pediatric precision medicine because it enables individualized dosing, complex film architectures, and on-demand production [9] [13] [16] [62]. Nevertheless, issues related to manufacturing throughput, quality assurance, regulatory acceptance, and cost-effectiveness must be addressed before widespread clinical implementation. Future progress is likely to involve hybrid manufacturing strategies that combine the scalability of conventional methods with the personalization capabilities of advanced printing technologies [9] [13] [62].
Table 4 : Key Insights of ODF’s
|
Section |
Key Insights |
Citations |
|
Mucosal Permeability |
Pediatric mucosa thinner/ more permeable than adults; enhances absorption and risk |
[1] [4][8] [10] [49] [52] |
|
PK Impact |
Rapid disintegration → higher Cmax/ lower Tmax; risk mitigated by SR microparticles |
[2] [4] [7][11] [51][52] |
|
First-Pass Avoidance |
Buccal/sublingual delivery can bypass liver metabolism—increases bioavailability |
[33][48] [49] [52] [54] |
|
IVIVC |
Challenging dueto age-dependent oral physiology/dynamic conditions |
[2] [4] [10][11] [49] [55] |
|
Film Polymers |
Pullulan/HPMC/PVA/PEO/cellulose ethers preferred; selection based on safety/mechanical needs |
[1] [7] [8] [11][17] |
|
Plasticizers |
Glycerol/sorbitol/PEG optimize flexibility but must balance tackiness/stability |
[1] [17] [33] [49] [57] |
|
Taste Masking |
Cyclodextrins/nanoparticles/SR microparticles/pH-sensitive polymers |
[2][4] [6] [8] [33][58] |
|
Excipients |
Avoid ethanol/parabens/high-risk surfactants/permeation enhancers unless proven safe |
[6] [10] [12] [33] [59] |
|
Drug Candidates |
Low-dose/stable/potent APIs best suited; BCS I preferred |
[2] [7][4] [11] [33] [51] |
10. Advanced Formulation and Drug Incorporation Strategies
Advanced formulation strategies are expanding the therapeutic scope of pediatric ODFs beyond conventional immediate-release systems. By integrating nanotechnology, amorphous drug delivery systems, and multilayer architectures, ODFs can overcome challenges related to poor solubility, limited drug loading, and complex dosing requirements. However, these innovations often increase formulation complexity and impose additional stability and manufacturing challenges.
10.1 Nanoparticles and Nanocomposites
Nanotechnology-based approaches have emerged as effective strategies for improving the performance of poorly water-soluble drugs in ODFs. Incorporation of nanocrystals, nanosuspensions, and polymeric nanoparticles increases surface area and dissolution rate, thereby enhancing drug release and bioavailability [3] [7] [14] [33].
Beyond solubility enhancement, nanoparticle-loaded ODFs can be designed to provide modified or extended drug release, expanding their applicability to pediatric therapies requiring prolonged exposure[3] [14] [33]. Nevertheless, increasing nanoparticle content may adversely affect film flexibility, tensile strength, and uniformity, highlighting the need to balance biopharmaceutical benefits with acceptable mechanical properties[14] [33] [35].
A key limitation is that improvements demonstrated in vitro do not always translate directly into predictable clinical outcomes, emphasizing the need for further in vivo evaluation in pediatric populations.
10.2 Amorphous Solid Dispersions (ASDs)
Amorphous solid dispersions (ASDs) are increasingly incorporated into ODFs to improve the dissolution of poorly soluble drugs. Technologies such as hot-melt extrusion (HME), hot-melt pressure extrusion (HMPE), and fused deposition modeling (FDM) enable direct fabrication of ASD-containing films with enhanced drug release characteristics [3] [39] [50]
Studies involving poorly soluble antipsychotics, including olanzapine and aripiprazole, have shown substantially faster dissolution from ASD-based ODFs compared with conventional solvent-cast formulations [3] [39] [50]This improvement is primarily attributed to the higher apparent solubility and molecular dispersion of the drug within the polymer matrix.
However, the thermodynamic instability of amorphous systems remains a major concern. Polymers such as PVA and poloxamers can stabilize the amorphous state, but strict humidity control is required to prevent recrystallization during storage and maintain long-term performance [3] [39] [50].
10.3 Layered and Fixed-Dose Combination Films
Multilayer and compartmentalized ODFs provide a versatile platform for addressing complex therapeutic requirements. By physically separating functional components, these systems can accommodate incompatible drugs, combine multiple release profiles, and integrate local and systemic therapy within a single dosage form [8] [9] [11] [33].
This approach is particularly valuable in pediatric medicine, where polypharmacy and individualized treatment regimens are common. Layer-specific design enables independent control of drug release, taste masking, and mucoadhesion, improving both therapeutic performance and patient acceptability [8] [11] [33].
A notable example is topiramate sustained-release microparticle-loaded ODFs, which combine rapid oral disintegration with prolonged systemic drug release, achieving pharmacokinetic profiles comparable to commercial extended-release formulations [8]. Similarly, 3D-printed multilayer mucoadhesive films containing clobetasol have demonstrated prolonged local retention with reduced systemic exposure, highlighting the potential of spatially engineered film architectures for targeted therapy [16].
Despite their advantages, multilayer systems involve more complex manufacturing processes and quality-control requirements than conventional monolayer films, which may limit large-scale implementation.
Critical Perspective
Advanced drug incorporation strategies have transformed ODFs from simple fast-dissolving dosage forms into multifunctional delivery platforms. Nanoparticles and ASDs effectively address solubility limitations, while multilayer architectures enable controlled release, drug combination, and targeted delivery[8] [33] [50]. However, these benefits are frequently accompanied by increased formulation complexity, stability concerns, and manufacturing challenges.
Current evidence demonstrates strong pharmaceutical potential, but pediatric clinical validation remains limited. Future development should focus on balancing technological sophistication with stability, scalability, regulatory feasibility, and age-appropriate safety requirements to facilitate successful clinical translation [16] [39] [50].
11. Evaluation and Characterization of Orodispersible Films
Comprehensive characterization of ODFs is essential to ensure product quality, dose accuracy, patient acceptability, and regulatory compliance. For pediatric formulations, evaluation extends beyond conventional pharmaceutical testing and must account for age-appropriate handling, rapid disintegration, palatability, and precise dosing requirements.
11.1 Physical and Mechanical Characterization
Mechanical integrity is critical for ensuring that films can withstand manufacturing, packaging, transportation, and administration without damage. Key quality attributes include thickness, weight uniformity, tensile strength, elongation at break, and folding endurance [11] [13] [35] [50].
Film composition significantly influences mechanical performance. Increased drug loading, particularly with dispersed particulate systems, may reduce flexibility and tear resistance by disrupting polymer matrix continuity [35]. In addition, manufacturing conditions can markedly affect film properties; for example, layer-by-layer drying during 3D printing influences internal structure, mechanical strength, and flexibility [9].
Therefore, mechanical characterization should balance robustness with the flexibility required for safe and acceptable pediatric administration.
11.2 Disintegration and Dissolution Testing
Rapid disintegration is a defining feature of ODFs and a key determinant of patient acceptability. Most formulations are designed to disintegrate within seconds to approximately 1–2 minutes using limited saliva volumes. Electrospun films may disintegrate within one second, whereas solvent-cast and printed films typically require 20–100 seconds depending on formulation and structure [7] [13] [9] [35] [39] [50].
Despite its importance, standardized disintegration testing for ODFs remains insufficiently established. Current methods often vary across studies, and disintegration behavior is strongly influenced by film thickness, porosity, and polymer composition]] [11] [9] [13][39].
Dissolution testing is particularly relevant for formulations containing nanostructured systems or amorphous solid dispersions, where enhanced drug release is a primary objective. Many printed ASD-based ODFs achieve more than 80% drug release within minutes, demonstrating significant improvements in dissolution performance [3] [7] [39].
11.3 Drug Content Uniformity
Content uniformity is especially critical for pediatric ODFs because small dosing deviations can have significant clinical consequences, particularly for low-dose and narrow therapeutic index drugs [11] [13].
Solvent casting can provide acceptable dose uniformity when mixing and drying processes are carefully controlled. However, high drug loading and particle aggregation may compromise dose distribution [14] [35] [50]. Printing technologies, including inkjet printing, 3D printing, and micro-dispensing, offer superior dose precision through direct control of deposited material and often outperform conventional extemporaneous formulations [13] [15] [56] [62].
The growing interest in personalized medicine has also driven the development of non-destructive, in-line analytical tools capable of monitoring dose accuracy during manufacturing, supporting real-time quality control of individualized ODFs [11].
11.4 Taste Evaluation Techniques
Palatability is a major determinant of pediatric adherence and therefore a critical quality attribute of ODFs. Various formulation approaches, including cyclodextrin complexation, maltodextrin incorporation, and solubilization strategies, have demonstrated effectiveness in reducing bitterness and improving sensory acceptance [33] [61].
Electronic tongue systems have emerged as valuable tools for objective taste assessment. These systems enable comparison of taste-masking strategies and have shown good correlation with reductions in perceived bitterness, reducing reliance on extensive pediatric sensory testing [61].
Advanced approaches, including multilayer films and dedicated taste-masking layers, are being investigated to further improve palatability; however, their clinical effectiveness and manufacturing feasibility require additional validation [9] [11] [33] [56].
Critical Perspective
Current evaluation methods effectively characterize the physical, mechanical, and biopharmaceutical performance of ODFs; however, significant challenges remain. Standardized disintegration and dissolution methodologies specific to pediatric ODFs are lacking, limiting cross-study comparisons and regulatory harmonization [11] [39]. Similarly, while printing technologies have substantially improved dose precision, robust real-time quality control systems are still evolving [11] [62].
Future characterization strategies should integrate biorelevant testing, advanced analytical tools, and patient-centered assessments to ensure that pediatric ODFs deliver consistent performance, accurate dosing, and acceptable sensory properties in real-world use [11] [13] [61].
12. Quality, Stability, and Packaging
12.1 Critical Quality Attributes (CQAs)
The quality of pediatric ODFs is defined by a combination of pharmaceutical and patient-centered attributes. Key CQAs include content uniformity, mechanical integrity, disintegration time, dissolution performance, residual solvent levels, and microbiological quality [1] [11] [49] [59]. These parameters directly influence product safety, efficacy, and consistency.
For pediatric applications, conventional quality metrics alone are insufficient. Patient-centered attributes such as taste, mouthfeel, flexibility, and stickiness are equally important because they strongly influence acceptability and adherence .Recent research has emphasized the use of biorelevant in vitro tools that simulate oral cavity conditions to better predict real-world performance in children [1] [31].
A major challenge is balancing rapid disintegration with adequate mechanical strength and sensory acceptability, as improvements in one attribute may negatively affect another.
12.2 Stability and Moisture Protection
ODFs are inherently susceptible to environmental moisture because of their thin structure and hydrophilic polymer composition [1] [49] [50]. Moisture uptake can cause film softening, sticking, loss of mechanical integrity, and changes in disintegration behavior. In advanced systems such as electrospun and ASD-based films, moisture may also trigger drug recrystallization, reducing dissolution performance and bioavailability [1] [49] [50].
Stability is therefore highly dependent on appropriate polymer selection, optimized plasticizer concentration, and effective moisture control strategies [1] [3] [49] [59]. High-barrier packaging systems, particularly foil–foil blisters and moisture-resistant sachets, are considered essential for maintaining product quality throughout shelf life [1] [49] [59].
Although promising stability data have been reported for several formulations, long-term stability remains a critical challenge, particularly for nanostructured and amorphous drug delivery systems.
12.3 Packaging for Pediatric ODFs
Packaging serves functions beyond product protection. In pediatric ODFs, it contributes to dose accuracy, microbiological safety, storage stability, and ease of administration [49] [11] [59].
Individually packaged dosage units, such as sachets and blisters, are preferred because they minimize contamination risk and facilitate accurate dosing by caregivers [49] [11] [59]. Patient-centric design principles further recommend packaging that is child-attractive while remaining tamper-resistant and easy for caregivers to open [12] [49] [31].
However, packaging complexity must be balanced against manufacturing cost and environmental sustainability, both of which are increasingly important considerations in pharmaceutical development.
13. Regulatory Considerations
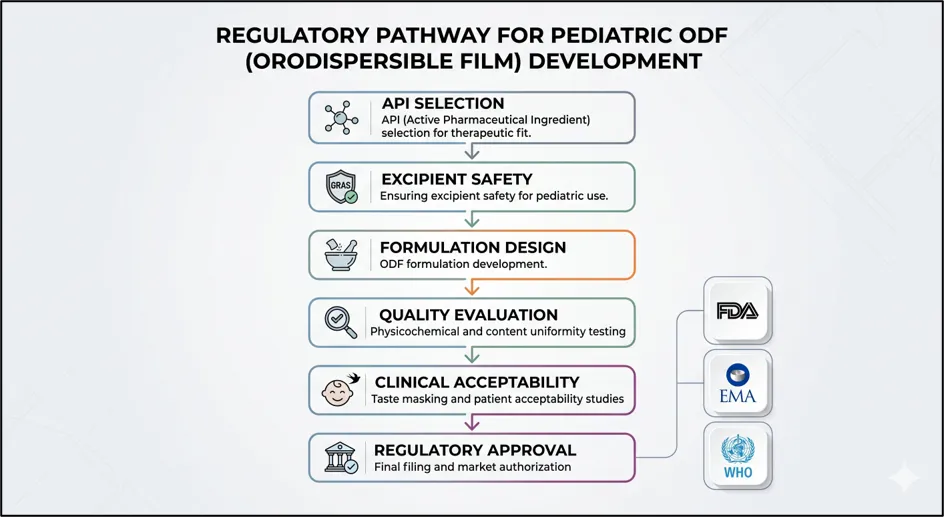
Figure 6 : Regulatory Pathway for ODF’s
13.1 Regulatory Expectations (FDA and EMA)
ODFs are generally regulated within the categories of oral soluble or oromucosal dosage forms. Regulatory requirements are guided by relevant pharmacopoeial standards and include assessment of content uniformity, mechanical properties, disintegration, dissolution, stability, and microbiological quality [57] [59].
For pediatric products, regulatory agencies increasingly expect evidence of palatability, swallowability, and overall acceptability in addition to conventional pharmaceutical quality testing [12] [36] [49] [57]. This reflects a growing recognition that clinical success in children depends not only on pharmacokinetic performance but also on patient adherence.
13.2 Bioequivalence and Clinical Evaluation
For systemically acting ODFs, bioequivalence is generally established using conventional pharmacokinetic endpoints and comparison with an appropriate reference product Several ODF platforms, including maltodextrin-based systems, have demonstrated bioavailability comparable to conventional oral formulations [36] [57].
Advanced formulations further illustrate the versatility of ODF technology. For example, topiramate sustained-release ODFs containing dual-coated microparticles achieved bioequivalence to a marketed extended-release product while retaining rapid oral disintegration [8].
Clinical acceptability studies in infants and preschool children consistently report high caregiver and patient acceptance, supporting the suitability of ODFs as age-appropriate dosage forms [2] [12]. Nevertheless, clinical evaluation remains heavily focused on bioequivalence rather than long-term therapeutic outcomes.
13.3 Current Regulatory Gaps
Despite increasing commercial interest, several regulatory challenges remain unresolved.
Major gaps include:
Addressing these issues will be essential for the broader adoption of advanced and personalized ODF platforms.
14. Marketed Products and Clinical Evidence
14.1 Available ODF Products
A growing number of prescription and over-the-counter ODF products are commercially available, including formulations containing ondansetron, sildenafil, analgesics, and nutraceutical ingredients [3] [36] [59]. Several products are either suitable for or specifically intended for pediatric use.
Maltodextrin-based ODF platforms have demonstrated broad applicability across multiple APIs, highlighting the versatility of film-based drug delivery systems [36].
14.2 Clinical Findings
Clinical studies generally support the acceptability and feasibility of ODFs in pediatric populations.
Key findings include:
These findings suggest that the primary clinical value of ODFs may lie in improving adherence and usability rather than substantially altering pharmacokinetic performance.
14.3 Limitations of Current Clinical Evidence
Despite encouraging results, the clinical evidence base remains relatively limited.
Current gaps include:
Consequently, many assumptions regarding long-term clinical benefits remain inadequately validated.
15. Emerging Trends and Future Directions
Orodispersible films (ODFs) are increasingly evolving from conventional age-appropriate formulations into platforms for personalized pediatric pharmacotherapy. Advances in additive manufacturing, digital production, and real-time quality control have expanded their potential beyond simple immediate-release systems. However, successful clinical translation will depend on overcoming challenges related to drug loading, regulatory acceptance, and long-term safety.
15.1 Personalized Dosing Platforms
Additive manufacturing technologies, including 2D printing, 3D printing, direct powder extrusion, and semi-solid extrusion, enable precise dose customization and flexible strength adjustment, addressing the variability of pediatric dosing requirements [9] [13] [15] [16] [62] [65] [66]. These approaches often provide superior dose accuracy and content uniformity compared with conventional dose manipulations [13] [15]. Nevertheless, printable drug candidates remain limited by constraints such as solubility, thermal stability, and achievable drug loading [51].
15.2 Digital and On-Demand Manufacturing
The integration of ODF manufacturing into hospital and pharmacy settings is becoming increasingly feasible through digital workflows and point-of-care production systems [17] [13] [66] [65]. Emerging technologies such as micro-dispensing allow accurate on-demand fabrication with predictable dose–area relationships [62]. Furthermore, combining machine learning with near-infrared spectroscopy and machine vision offers opportunities for automated dose verification and real-time quality assessment [67]. Despite these advances, standardization and regulatory oversight remain essential for widespread implementation.
15.3 Integration of QbD and PAT
Quality by Design (QbD) principles are increasingly being applied to ODF development, emphasizing critical quality attributes such as disintegration, mechanical performance, taste, and dose uniformity [1] [11] [14] [33]. In parallel, Process Analytical Technology (PAT) tools, including NIR spectroscopy, machine vision, and online content analysis, are being explored for real-time process monitoring and quality assurance [11] [14] [33] [67]. These technologies are particularly valuable for personalized and small-batch manufacturing, where conventional end-product testing may be impractical.
Research Gaps and Future Directions
Several barriers continue to limit the broader adoption of pediatric ODFs. Drug-loading capacity remains insufficient for many high-dose or poorly soluble APIs, necessitating advanced strategies such as nanoparticles, multilayer films, and repeated printing processes [7] [14] [33] [51]. Long-term safety data for novel excipients, thiomers, and nanostructured systems are also limited, particularly in pediatric populations[2] [7] [9] [16] [33]. Moreover, most studies focus on formulation development and pharmacokinetics, whereas evidence linking ODFs to improved adherence, clinical outcomes, and cost-effectiveness remains scarce [2] [8] [12] [13]. Regulatory frameworks for personalized, digitally manufactured ODFs are still evolving, with unresolved issues related to quality assurance, data integrity, and manufacturing responsibility [11] [13] [17] [67].
Critical Perspective
The future of pediatric ODFs lies in the convergence of personalized manufacturing, digital quality control, and patient-centric formulation design. While printing technologies and advanced analytical tools offer unprecedented opportunities for individualized therapy, their clinical impact will depend on robust regulatory frameworks, long-term safety evaluation, and evidence demonstrating meaningful improvements in patient outcomes. Future research should therefore focus on translating technological innovation into clinically validated and scalable pediatric medicines [11] [13] [67]
CONCLUSION
Orodispersible films (ODFs) have emerged as a promising and patient-centric drug delivery platform capable of addressing many of the long-standing challenges associated with pediatric pharmacotherapy. Their rapid disintegration, ease of administration without water, improved swallowability, dose flexibility, enhanced palatability, and potential for buccal drug absorption make them particularly suitable for infants, children, and patients with dysphagia. Compared with conventional oral dosage forms, ODFs offer significant advantages in terms of patient compliance, caregiver convenience, and therapeutic acceptability.
Recent advances in formulation science, including the use of novel film-forming polymers, taste-masking technologies, nanotechnology-based drug delivery systems, amorphous solid dispersions, and multilayer film architectures, have substantially expanded the therapeutic potential of ODFs. Furthermore, emerging manufacturing approaches such as electrospinning, inkjet printing, and three-dimensional printing are paving the way for personalized pediatric medicines with precise and individualized dosing.
Despite these advances, several challenges continue to limit the widespread clinical adoption of ODFs. Limited drug-loading capacity, moisture sensitivity, complex taste-masking requirements, insufficient pediatric-specific pharmacokinetic data, excipient safety concerns, and the absence of harmonized regulatory guidelines remain significant barriers. Additionally, greater efforts are needed to establish standardized evaluation methods, robust in vitro–in vivo correlations, and long-term clinical evidence supporting efficacy, safety, and patient acceptability.
Overall, ODFs represent a transformative and versatile dosage form with the potential to revolutionize pediatric drug delivery. Continued research focusing on advanced formulation strategies, scalable manufacturing technologies, pediatric-specific safety assessments, and regulatory standardization will be essential to facilitate their successful translation from laboratory innovation to routine clinical practice. With these developments, ODFs are expected to play a central role in the future of personalized and age-appropriate pediatric medicine.
REFERENCES


Shivani Sharma, Dr. Bharat Jain, Orodispersible Films as a Child-Centric Revolution in Paediatric Medicine, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 414-446. https://doi.org/10.5281/zenodo.21140517
 10.5281/zenodo.21140517
10.5281/zenodo.21140517