
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SEMS Mahavir Institute of Pharmacy, Nashik.
Colonic diseases — inflammatory bowel disease, colorectal malignancy, and infectious colitis — require targeted pharmacological intervention at the large intestinal mucosa. Biologic therapeutics such as monoclonal antibodies, recombinant proteins, nucleic acid-based therapies, and extracellular vesicles possess excellent target specificity but face near-complete oral bioavailability failure owing to the sequential degradation imposed by the gastrointestinal tract: acid-mediated unfolding, enzymatic proteolysis, mucus barrier entrapment, and epithelial tight junction restriction. pH-responsive hydrogels exploit the predictable rise in intraluminal pH from the stomach (pH 1.2–2.0) to the ileocolonic junction (pH 6.8–7.4) to achieve site-selective colonic biologic release. These ionisable, crosslinked polymer networks remain structurally compact and protective under acidic gastric conditions, then undergo thermodynamically driven swelling through Donnan osmotic pressure generation and electrostatic repulsion upon carboxylate group ionisation at colonic pH, enabling controlled macromolecular diffusion. This comprehensive review covers the mechanistic basis of pH-responsive swelling from thermodynamic and kinetic perspectives — including Flory-Rehner theory, Donnan osmotic swelling, mesh size dynamics, and Korsmeyer-Peppas drug release modelling — alongside polymer chemistry, formulation design, figure-based schematic analysis, and clinical translation. Ten summary tables and multiple schematic figure descriptions organise GI environmental parameters, polymer benchmarks, swelling thermodynamics, drug release kinetics, biologic delivery outcomes, fabrication approaches, crosslinking strategies, characterisation methods, clinical evidence, and translational challenge-solution pairings
The colonic mucosa holds a dual therapeutic significance rarely encountered in any other organ: it is simultaneously the primary site of pathological injury in inflammatory bowel disease and a critical anatomical target for loco-regional gene-based therapies in colorectal carcinoma. This convergence has driven decades of pharmaceutical research into colon-targeted drug delivery systems, yet the reliable and efficient delivery of intact biologic drugs to this site through oral administration remains among the most technically demanding problems in contemporary pharmaceutical science.
Biologic medicines — monoclonal antibodies, recombinant cytokines, small interfering RNA, and mesenchymal stem cell-derived extracellular vesicles — have fundamentally changed the treatment landscape for moderate-to-severe IBD since infliximab entered clinical practice in 1998. Successive generations of anti-TNF-α, anti-integrin, anti-IL-12/23, and JAK-inhibitor agents have progressively expanded the therapeutic armamentarium, achieving mucosal healing rates previously unattainable. Yet these agents all share a pharmacological paradox: systemic administration is required for a disease whose pathological activity is concentrated within the colonic mucosa. High circulating drug concentrations needed to saturate mucosal receptors simultaneously suppress systemic immune surveillance, elevating risks of opportunistic infections, lymphoma, and demyelinating disorders.
pH-responsive hydrogels capitalise on a fundamental physiological asset — the predictable longitudinal pH gradient of the gastrointestinal tract. Anionic polymer networks bearing ionisable carboxylic acid groups remain protonated, compact, and structurally protective throughout the acidic gastric and upper intestinal environment, then undergo progressive ionisation-driven swelling as luminal pH rises toward the ileocolonic junction value of approximately 6.8–7.4. The resulting network expansion enables controlled diffusion of encapsulated biologic payload at the desired colonic target without requiring any external physical, chemical, or electronic triggering mechanism. This review provides a comprehensive, mechanistically deep, and clinically contextualised synthesis of the field, incorporating ten summary tables and detailed schematic figure descriptions.
2. Gastrointestinal Physiology and Pathological Microenvironment
2.1 Longitudinal pH Profile and Its Pharmacological Significance
A thorough understanding of luminal pH values, their variability, and their biological consequences at each gastrointestinal segment is essential for rational pH-responsive hydrogel design. Table 1 consolidates these parameters.
Table 1. Intraluminal pH, transit characteristics, and drug delivery significance at successive gastrointestinal anatomical regions.
|
Anatomical Region |
Luminal pH |
Residence Duration |
Delivery Design Implications |
|
Stomach (fasted) |
1.2–2.0 |
0.5–2 h |
Outer hydrogel must withstand acid; biologic at risk of unfolding below pH 3.0 |
|
Stomach (postprandial) |
3.0–5.0 |
1–4 h |
Food transiently buffers acid; enteric coatings may partially swell; robust second barrier needed |
|
Duodenum |
5.5–6.5 |
15–30 min |
Pancreatic proteases active; L100-55 dissolution threshold reached; S100 still intact |
|
Jejunum / Ileum |
6.5–7.2 |
2–4 h |
Brush-border peptidases active; L100 may begin dissolving; S100 coat remains protective |
|
Ileocaecal junction |
6.8–7.4 |
Variable |
Primary trigger zone for S100 dissolution and anionic hydrogel swelling onset |
|
Ascending/transverse colon |
6.5–7.5 |
6–24 h |
Highest microbial density; ROS elevated in IBD; extended transit supports prolonged biologic release |
|
Sigmoid/descending colon |
7.0–8.0 |
Up to 48 h |
Highest pH; complete enteric coat dissolution; suitable for sustained colonic biologic release |
Gastric pH in the fasted adult ranges from 1.2 to 2.0, generated by parietal cell H⁺/K⁺-ATPase proton secretion. This highly acidic milieu constitutes the primary threat to biologic integrity, as most globular proteins undergo irreversible tertiary structure collapse below pH 3.0 through protonation of buried histidine, aspartate, and glutamate residues that normally stabilise the hydrophobic core. RNA molecules undergo acid-catalysed hydrolysis of the phosphodiester backbone with a half-life measured in seconds at pH 1.2. Upon pyloric evacuation, pancreatic bicarbonate secretion raises duodenal pH to 5.5–6.5 within minutes; jejunal and ileal pH progresses to 6.5–7.2. The ileocaecal junction, where pH reaches 6.8–7.4, represents the pharmacologically defined trigger zone for colonic delivery systems. Clinically significant variability arises from proton pump inhibitor therapy, achlorhydria, and active IBD-associated lactic acid accumulation in the inflamed colonic mucosa.
2.2 IBD Pathological Microenvironment
Active IBD creates a distinctive colonic microenvironment that differs from healthy tissue across multiple physicochemically relevant dimensions. Activated neutrophils and macrophages generate reactive oxygen species — principally H₂O₂, superoxide (O₂•⁻), and hypochlorite (HOCl) — at concentrations 10- to 100-fold above healthy mucosal baselines through NADPH oxidase-mediated pathways. This elevated ROS burden simultaneously constitutes a therapeutic target and a secondary formulation trigger for dual pH/ROS-responsive carriers. Mucosal permeability is pathologically increased through redistribution of claudin-1, occludin, and ZO-1 tight junction proteins, creating paracellular gaps that may paradoxically facilitate macromolecular absorption from colonic lumen to submucosal compartment — a feature exploited by site-selective biologic delivery systems. IBD dysbiosis reduces populations of polysaccharide-degrading Bacteroidetes, compromising the enzymatic lability of pectin and guar gum matrices that rely on microbial pectinase and galactomannanase for colonic release.
3. Mechanisms of pH-Responsive Swelling and Drug Release
Understanding the mechanistic basis of pH-triggered swelling and drug release in hydrogel systems is fundamental to rational formulation design at the M.Pharm level. The release behaviour of pH-responsive hydrogels is governed by a sequence of interconnected thermodynamic, electrostatic, and kinetic phenomena that collectively determine the magnitude, rate, and selectivity of biologic payload liberation at the target GI site.
3.1 Thermodynamic Framework: Flory-Rehner Theory
The equilibrium swelling behaviour of a crosslinked polymer network in a solvent is described by the Flory-Rehner theory, which recognises two opposing contributions to the total free energy of swelling. The first is the free energy of mixing (ΔGmix), which is negative (favourable) when the polymer-solvent interaction parameter χ (Flory-Huggins parameter) is sufficiently low — this thermodynamic component drives the polymer to absorb solvent. The second is the elastic free energy of the crosslinked network (ΔGelastic), which is positive (unfavourable) because swelling stretches the polymer chains between crosslinks, storing elastic energy analogous to a mechanical spring. At equilibrium swelling, these two contributions exactly balance:
ΔGtotal = ΔGmix + ΔGelastic = 0
For pH-responsive anionic hydrogels, the critical insight is that ionisation of carboxylic acid groups above their pKa dramatically lowers the effective χ parameter by introducing electrostatic repulsion between adjacent polymer chain segments — repulsion that the Flory-Huggins model treats as an additional driving force for chain expansion. The Flory-Rehner equation for the equilibrium polymer volume fraction in the swollen network (v2,s) — which is inversely proportional to the degree of swelling — is given by:
[ln(1 − v2,s) + v2,s + χv2,s²] + V₁/Vc × (v2,s^(1/3) − v2,s/2) = 0
where V₁ is the molar volume of the solvent and Vc is the molar volume of the polymer between crosslinks. At gastric pH, carboxylate groups are protonated (R-COOH), χ remains high, and v2,s is large (low swelling — compact network). At colonic pH (above pKa), progressive deprotonation generates R-COO⁻ anions, electrostatic repulsion lowers effective χ, and v2,s falls dramatically — corresponding to large-scale swelling. The mesh size (ξ) of the swollen network, which governs the diffusion of encapsulated biologic molecules, scales with v2,s according to:
ξ = v2,s^(−1/3) × (r̄0²)^(1/2)
where r̄0 is the root-mean-square end-to-end distance of the freely jointed polymer chain between crosslinks. For a biologic with hydrodynamic radius rs to diffuse through the network, ξ must exceed rs. For IgG antibodies (rs ≈ 5–8 nm), ξ must reach approximately 10 nm at colonic pH — a design criterion that directly specifies the required crosslink density.

Figure 1. Schematic representation of pH-triggered swelling in anionic hydrogels. At gastric pH, carboxylic acid groups remain protonated (R-COOH), maintaining a compact network with mesh size smaller than the biologic hydrodynamic radius. Upon reaching colonic pH, ionisation generates fixed negative charges (R-COO⁻), electrostatic repulsion drives rapid water uptake and network expansion, and mesh size exceeds the critical threshold for macromolecular diffusion. ESR = equilibrium swelling ratio. The double arrows indicate the reversibility of the swelling transition — relevant to self-healing Schiff base hydrogels — while the one-way arrow indicates the physiological context of irreversible transit toward the colon.
3.2 Donnan Osmotic Pressure and Electrostatic Swelling Driving Force
The Donnan membrane equilibrium provides the quantitative electrostatic framework for understanding swelling in ionisable hydrogels. When a polyelectrolyte hydrogel bearing fixed charges (ionised carboxylate groups, R-COO⁻) is immersed in an electrolyte solution, mobile counterions (primarily Na⁺) are preferentially concentrated within the gel interior relative to the external solution, while mobile co-ions (Cl⁻) are excluded by electrostatic repulsion. This unequal ion distribution creates a Donnan osmotic pressure (π) across the gel-solution interface, which drives water into the hydrogel network:
π = RT × Σi (ci,gel − ci,solution)
where ci,gel and ci,solution are the molar concentrations of mobile ion species i inside and outside the gel, R is the gas constant, and T is absolute temperature. At gastric pH, where carboxylate groups are protonated, there are no fixed charges, no Donnan effect, and no osmotic swelling driving force beyond simple polymer-solvent mixing — explaining why anionic hydrogels remain compact in the stomach. As pH rises above the polymer pKa at the ileocolonic junction, progressive deprotonation introduces fixed negative charges, the Donnan potential increases, counterion concentration gradient between gel interior and external GI fluid grows, and osmotic water influx drives dramatic network expansion.
The magnitude of Donnan swelling depends critically on the degree of ionisation (α), which is governed by the Henderson-Hasselbalch relationship:
α = 1 / (1 + 10^(pKa − pH))
At colonic pH 7.4, a polymer with pKa 3.5 (e.g., alginate carboxylates) exhibits α ≈ 1.0 (essentially complete ionisation), while at gastric pH 1.2, α ≈ 10⁻²·³ (< 1% ionisation). This sharp ionisation transition across the GI pH gradient translates directly into the dramatic swelling selectivity that makes anionic hydrogels effective colonic delivery vehicles. For polymer systems with pKa values in the range of 4.5–6.0 (e.g., PAA, Carbopol), partial ionisation begins in the jejunum (pH 6.5) — explaining the tendency toward premature small intestinal swelling with these materials and the rationale for using Eudragit® S100 (which dissolves only above pH 7.0) as an outer coating to delay swelling onset.

Figure 2. Degree of ionisation (α) of key anionic polymers as a function of gastrointestinal luminal pH, calculated using the Henderson-Hasselbalch equation. Alginate and pectin (pKa ~3.4–3.5) reach near-complete ionisation by duodenal pH but their Ca²⁺-crosslinked networks rely on ionic stability rather than protonation to maintain integrity. PAA/Carbopol (pKa ~5.0) shows partial ionisation (50%) in the jejunum, explaining premature swelling tendency. Eudragit® S100 undergoes film dissolution — not ionisation-driven swelling — above pH 7.0, providing the most selective colonic trigger among clinically established materials.
3.3 Mesh Size Dynamics and Macromolecular Diffusion
The mesh size (ξ) of a swollen hydrogel network is the single most critical structural parameter governing whether an encapsulated biologic can diffuse through the matrix. It can be estimated from the Flory-Rehner equation or from mechanical data using the rubber elasticity theory:
ξ = (RT / G')^(1/3) × v2,s^(−1/3)
where G' is the storage modulus measured by oscillatory rheology and v2,s is the polymer volume fraction in the swollen state. The effective diffusion coefficient of a spherical biologic molecule with Stokes radius rs through the hydrogel network is described by the Ogston-type hindered diffusion model:
Deff / D0 = exp(−π × rs² / ξ²)
This exponential dependence on (rs/ξ)² has profound practical consequences: even a modest increase in mesh size from pH-triggered swelling produces a large amplification in biologic diffusivity. For example, if ξ increases from 4 nm (gastric pH) to 12 nm (colonic pH) — a 3-fold change — and rs for a 30 kDa protein is 2 nm, then Deff/D0 increases from exp(−π × 4/16) ≈ 0.46 to exp(−π × 4/144) ≈ 0.92, nearly doubling the fractional diffusivity. For IgG antibodies (rs ≈ 7 nm), the same mesh expansion switches the system from essentially impermeable (Deff/D0 ≈ exp(−π × 49/16) ≈ 0.000055) to moderately permeable (Deff/D0 ≈ exp(−π × 49/144) ≈ 0.34) — a 6,000-fold increase in effective diffusivity, explaining the dramatic pH-sensitivity of biologic release from well-designed hydrogel systems.
3.4 Drug Release Kinetic Models
Following pH-triggered swelling and network expansion, the kinetics of biologic payload release from the hydrogel matrix are described by a hierarchy of mathematical models of increasing mechanistic complexity. Selection of the appropriate model — based on goodness of fit (r² > 0.99) and mechanistic plausibility — is an important component of hydrogel formulation characterisation at the M.Pharm level. Table 9 summarises the principal kinetic models with their equations, mechanistic interpretations, and specific relevance to pH-responsive hydrogel systems.
Table 9. Mathematical models for drug release kinetics from pH-responsive hydrogels, with mechanistic interpretations and hydrogel-specific relevance.
|
Kinetic Model |
Mathematical Equation |
Release Mechanism |
Relevance for pH-Responsive Hydrogels |
|
Zero-order |
Qt = Q0 + K0t |
Constant rate; independent of concentration |
Applicable to matrix systems releasing biologic at constant rate after pH-triggered swelling plateau; rarely achieved alone in swellable hydrogels |
|
First-order |
log Qt = log Q0 − K1t/2.303 |
Rate proportional to remaining drug concentration |
Governs early burst release of surface-adsorbed biologic from hydrogel before swelling equilibrium; common in alginate bead systems |
|
Higuchi model |
Qt = KH √t |
Diffusion-controlled from matrix |
Describes protein diffusion from swollen hydrogel matrix post pH-trigger; applicable when mesh size >> biologic hydrodynamic radius |
|
Korsmeyer-Peppas |
Mt/M∞ = Ktn |
n ≤ 0.45: Fickian diffusion; 0.45 < n < 0.89: anomalous; n = 0.89: Case-II (swelling-controlled); n > 0.89: Super Case-II |
Most widely applied to pH-responsive hydrogels; n value distinguishes diffusion- vs swelling-dominated release; biologic macromolecules typically show anomalous (non-Fickian) transport due to coupled swelling and diffusion |
|
Peppas-Sahlin |
Mt/M∞ = K1tm + K2t2m |
Separates Fickian diffusion (K1 term) from relaxation/swelling contribution (K2 term) |
Particularly useful for pH-responsive hydrogels where network relaxation (swelling-driven chain mobility changes) and molecular diffusion simultaneously govern release; K2/K1 ratio quantifies relative contribution of each mechanism |
|
Hixson-Crowell |
Q0^(1/3) − Qt^(1/3) = Kst |
Surface area-controlled erosion/dissolution |
Applicable to Eudragit® S100-coated systems where pH-triggered outer coating dissolution controls total surface area available for drug release; erosion-dominant mechanism |
The Korsmeyer-Peppas power law model (Mt/M∞ = Ktn) is the most widely applied kinetic framework for pH-responsive hydrogels because the diffusion exponent n directly distinguishes the dominant release mechanism without requiring knowledge of the diffusion coefficient or network geometry. For slab geometry — the relevant geometry for film-coated tablets and flat hydrogel matrices — n = 0.5 indicates Fickian diffusion (biologic concentration-gradient-driven), n = 1.0 indicates Case-II transport (swelling-rate-controlled, zero-order release), and 0.5 < n < 1.0 indicates anomalous (non-Fickian) transport where both diffusion and network swelling contribute to release. For biologic macromolecules with large hydrodynamic radii, anomalous transport (n values of 0.6–0.85) is the most commonly reported mechanism in pH-responsive alginate, chitosan, and PAA-based systems — consistent with the coupled swelling and diffusion processes governing their release. For cylindrical beads and spherical particles (the most common morphologies for oral colonic formulations), the critical n values shift to 0.45 (Fickian) and 0.89 (Case-II), and the Korsmeyer-Peppas equation is typically applied to only the first 60% of cumulative release (Mt/M∞ ≤ 0.60) to avoid artefacts from the late-phase depletion of drug reservoir.
The Peppas-Sahlin model, which deconvolutes total release into a pure Fickian diffusion term (K₁ × t^m) and a pure swelling relaxation term (K₂ × t^2m), is particularly informative for pH-responsive hydrogels where network relaxation — the time-dependent conformational rearrangement of polymer chains upon swelling — is an important kinetic process. The ratio K₂/K₁ quantifies the relative contribution of swelling-driven (Case-II) transport versus concentration-gradient-driven Fickian diffusion; a high K₂/K₁ ratio (> 1) identifies formulations where the rate of network swelling, rather than biologic diffusivity, is the rate-limiting step for payload release.
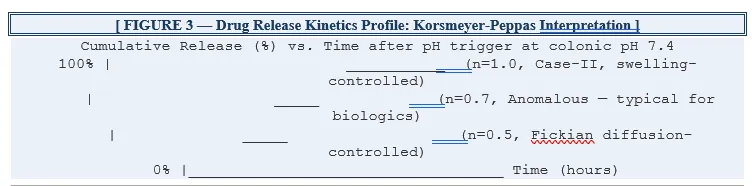
Figure 3. Schematic drug release profiles illustrating Korsmeyer-Peppas diffusion exponent interpretation for pH-responsive hydrogels at colonic pH (pH 7.4 trigger). n = 0.5 (Fickian) indicates biologic release is driven solely by concentration gradient diffusion through a stable swollen network; n = 0.7 (anomalous) represents the most common case for biologic macromolecules where coupled swelling and diffusion operate simultaneously; n = 1.0 (Case-II) indicates network swelling rate is rate-limiting, producing near-zero-order release. For IgG antibodies in alginate/chitosan systems, reported n values typically fall between 0.6 and 0.85.
3.5 Swelling Thermodynamics Summary
Table 10 consolidates the key thermodynamic and kinetic parameters governing pH-responsive hydrogel swelling and biologic release, providing a structured reference for formulation design decisions.
Table 10. Thermodynamic and kinetic parameters governing pH-responsive hydrogel swelling and macromolecular biologic release.
|
Theoretical Parameter |
Definition / Equation |
Physical Significance |
Impact on Biologic Release |
|
Equilibrium swelling ratio (ESR) |
ESR = (Ws − Wd) / Wd Ws = swollen mass; Wd = dry mass |
Quantifies total water uptake; reflects ionisation extent and osmotic driving force at given pH |
Higher ESR → larger mesh size → faster macromolecular diffusion; ESR ratio pH 7.4/1.2 defines trigger selectivity |
|
Polymer volume fraction (v2,s) |
v2,s = Vd / Vs Vd = dry volume; Vs = swollen volume |
Inversely proportional to swelling; decreases as crosslink density falls or ionisation increases |
Low v2,s (high swelling) increases mesh size; must not fall below threshold that causes biologic leaching before target site |
|
Flory-Rehner mesh size (ξ) |
ξ = v2,s^(−1/3) × (r̄0²)^(1/2) r̄0 = end-to-end distance of polymer chain |
Average pore diameter of swollen network; determines steric accessibility of biologic payload |
For IgG delivery: ξ must exceed ~10 nm (IgG hydrodynamic diameter) at colonic pH while remaining <5 nm at gastric pH to prevent premature release |
|
Flory-Huggins interaction parameter (χ) |
χ = Vs/RT × (δs − δp)² δs, δp = solubility parameters of solvent and polymer |
Quantifies polymer-solvent thermodynamic compatibility; lower χ = better swelling thermodynamics |
Anionic polymers exhibit lower effective χ above pKa due to electrostatic repulsion amplifying thermodynamic swelling driving force at colonic pH |
|
Donnan osmotic pressure (π) |
π = RT × Σ(ci,in − ci,out) ci = ion concentration inside/outside gel |
Osmotic pressure generated by fixed charges on ionised polymer chains retaining mobile counterions; major swelling driving force above pKa |
At colonic pH, ionised carboxylate groups accumulate Na⁺ counterions within network; resulting osmotic gradient drives water influx, rapid mesh expansion, and accelerated biologic diffusion |
|
Effective diffusion coefficient (Deff) |
Deff = D0 × exp(−π × rs² / ξ²) D0 = free solution diffusivity; rs = solute radius |
Actual diffusivity of biologic through swollen hydrogel network; strongly dependent on ratio of solute radius to mesh size |
Exponential dependence means small increases in mesh size (from pH-triggered swelling) produce large increases in biologic diffusion coefficient; explains rapid release onset at trigger pH |
3.6 Polymer-Specific pH-Response Mechanisms
3.6.1 Alginate: Ionotropic Gelation and pH-Triggered Decrosslinking
Sodium alginate forms physical hydrogel networks through cooperative coordination of Ca²⁺ ions with the carboxylate groups of guluronate (G-block) sequences in an antiparallel pairing arrangement — the egg-box model. At gastric pH, the Ca²⁺-guluronate coordination bonds are supplemented by protonation of carboxylate groups, which reduces electrostatic repulsion between chains and stabilises the junction zones. As luminal pH rises through the small intestine, progressive deprotonation of the mannuronate and guluronate carboxylates (pKa ~3.4) increases electrostatic repulsion within and between polymer chains, weakening junction zones. However, the Ca²⁺ coordination itself provides substantial structural integrity independent of protonation state — explaining why alginate beads frequently require phosphate ion-mediated Ca²⁺ chelation (which disrupts junction zones by competing for Ca²⁺) in addition to pH-triggered carboxylate ionisation for complete dissolution in the small intestine. This is the mechanism by which phosphate-buffered simulated intestinal fluid (SIF-USP) challenges alginate matrix integrity — and why Eudragit® S100 outer coating or chitosan inner layers are added to protect against premature SIF-induced dissolution.
3.6.2 Eudragit S100: Anionic Copolymer Dissolution Above pH 7.0
Eudragit® S100 is a random copolymer of methacrylic acid (MAA) and methyl methacrylate (MMA) in a 1:2 molar ratio. The MAA repeat units bear carboxylic acid groups with an apparent pKa of approximately 6.8–7.0 — shifted upward from the free acid value (~4.6) by the hydrophobic MMA microenvironment and the polyelectrolyte effect. Below pH 7.0, the MAA units are predominantly protonated, and the MMA hydrophobic segments maintain the polymer in a glassy, water-impermeable film state. Above pH 7.0, sufficient carboxylate ionisation occurs to generate electrostatic repulsion between chain segments and osmotic water influx into the film, leading to rapid film dissolution. The sharp dissolution threshold at pH 7.0 — experimentally confirmed by the absence of significant drug release below pH 6.8 in well-formulated Eudragit S100-coated systems — makes this polymer the most reliable pH trigger for ileocolonic targeting currently available.
3.6.3 Chitosan: Cationic pH Response and Polyelectrolyte Complex Behaviour
Chitosan's primary amine groups (pKa 6.2–6.5) protonate at acidic pH, making the polymer cationic, soluble, and swollen. At neutral-to-alkaline colonic pH, deprotonation causes chitosan to collapse and precipitate from solution. This inverse pH response is leveraged in polyelectrolyte complex (PEC) formation with anionic polymers such as alginate: the electrostatic pairing between alginate carboxylates (R-COO⁻) and chitosan ammonium groups (R-NH₃⁺) creates a stable polyelectrolyte complex that is resistant to dissolution across a wide pH range. As pH rises above 7.0 at the ileocolonic junction, two concurrent changes destabilise the PEC: (i) alginate carboxylate groups become fully ionised, generating repulsion that disrupts chain pairing; and (ii) chitosan amine groups begin deprotonating (above pKa 6.2), reducing the cationic charge density available for electrostatic pairing. The combination of these two effects produces a sharp dissolution transition at the ileocolonic pH — which is the mechanistic basis for the superior colon-selectivity of alginate-chitosan composite hydrogel beads compared to single-polymer systems.
4. pH-Responsive Polymers: Chemistry and Biologic Suitability
Polymer selection is the foundational formulation decision governing release threshold, network stability, biologic compatibility, and regulatory acceptability. Table 2 provides a comparative overview of the major polymer classes.
Table 2. Comparative properties of major pH-responsive polymers employed in colon-targeted biologic delivery hydrogels.
|
Polymer |
Origin |
Trigger pH |
Swelling at pH 7.4 |
Principal Strengths |
Notable Limitations |
|
Sodium alginate |
Natural, anionic |
pKa ~3.4 |
Very high (~99% water) |
Aqueous Ca²⁺ gelation; no solvent risk; biodegradable |
Phosphate-mediated premature dissolution; M/G batch variability |
|
Chitosan (native) |
Natural, cationic |
pKa ~6.2–6.5 |
Collapses at neutral pH |
Strong mucoadhesion; tight junction modulator; amine-rich for grafting |
Inverse pH response; must be blended for colon release |
|
Pectin (LM) |
Natural, anionic |
pKa ~3.5 |
Moderate–high |
Dual pH + pectinase enzymatic trigger; selective colonic degradation |
Dysbiotic IBD microbiome may reduce enzymatic reliability |
|
CMGG (modified guar) |
Semi-synthetic |
~4.5 |
High post-modification |
Galactomannanase lability; low cost; non-immunogenic |
pH-insensitive until modified; limited biologic loading data |
|
Hyaluronic acid |
Natural, anionic |
pKa ~3.0 |
High (crosslinked) |
CD44-receptor targeting of inflamed macrophages; ECM-mimetic |
Rapid hyaluronidase degradation; requires crosslinking |
|
Eudragit® S100 |
Synthetic, anionic |
Dissolves ≥pH 7.0 |
Film dissolution |
Clinically established; precise pH threshold; regulatory precedent |
Coating only; must combine with inner hydrogel for rate control |
|
Poly(acrylic acid)/Carbopol |
Synthetic, anionic |
pKa ~4.5–5.0 |
50–100× swelling |
Extreme swelling ratio; strong mucoadhesion; well characterised |
Premature jejunal swelling at pH 6.5; synthetic origin |
|
IAc–AAm nanogel |
Synthetic |
pKa ~2.9/~5.5 |
~10× vs gastric |
Intrinsic ROS scavenging (5× control); dual-function therapeutic + responsive |
Limited long-term toxicology; scalability unproven |
4.1 Natural Polysaccharides
Sodium alginate forms Ca²⁺-crosslinked beads under entirely aqueous, ambient-temperature conditions that impose minimal stress on co-encapsulated biologics. Encapsulation efficiency for model proteins via in situ gelation routinely exceeds 80%, with preserved biological activity after simulated gastric exposure documented in alginate-chitosan nanosphere systems. Chitosan, the only naturally derived cationic polysaccharide in broad pharmaceutical use, contributes mucoadhesion through electrostatic attraction to negatively charged mucin glycoproteins, paracellular tight junction opening through ZO-1 redistribution, and versatile chemical modification capacity. Thiolated chitosan forms disulfide bonds with mucin cysteine residues for covalent mucoadhesion of substantially greater duration than electrostatic attachment. Pectin provides dual-mechanism colon selectivity through pH-triggered swelling and selective pectinase degradation by colonic Bacteroidetes. Hyaluronic acid adds active CD44-receptor targeting to pH-triggered passive release, concentrating biologic delivery in inflamed macrophages and tumour cells.
4.2 Synthetic pH-Responsive Polymers
Eudragit® S100 occupies a unique position as the only pH-responsive polymer with documented regulatory approval history for colon-targeted delivery, its dissolution threshold at pH ≥7.0 providing a reliable trigger aligned with the ileocolonic junction. Crosslinked polyacrylic acid (Carbopol®) delivers the most dramatic swelling responses — 50- to 100-fold increase from gastric to intestinal pH — at the cost of swelling onset at jejunal pH (6.5), addressed by copolymerisation with hydrophobic monomers or IPN formation with enzymatically labile polysaccharides. Itaconic acid-acrylamide nanogels represent a multifunctional advance: pH-responsive swelling (10-fold between gastric and colonic pH) combined with intrinsic ROS-scavenging activity five times greater than control materials.

Figure 4. Schematic map of pH-responsive polymer behaviour across the gastrointestinal pH gradient. ICV = ileocaecal valve. Alginate swells at ileocolonic pH but may dissolve prematurely in phosphate-rich simulated intestinal fluid without outer coating protection. PAA/Carbopol begins swelling at jejunal pH (6.5), indicating risk of small intestinal biologic release. Eudragit® S100 remains intact as a film until pH 7.0 is reached at the ileocaecal valve, providing the most selective colonic trigger. Combining an Eudragit® S100 outer coat with an inner alginate hydrogel reservoir exploits the complementary properties of both systems.
5. Formulation Architecture, Crosslinking, and Biologic Loading
5.1 Crosslinking Strategy Comparison
The crosslinking strategy shapes every downstream performance characteristic. Table 6 provides a structured comparison.
Table 6. Comparison of crosslinking strategies for pH-responsive hydrogels used in colon-targeted biologic delivery.
|
Crosslinking Type |
Example Chemistry |
Gel Stability |
Biologic Safety Profile |
pH-Release Mechanism |
|
Ionotropic (physical) |
Ca²⁺ + alginate carboxylates |
Moderate; dissolves in phosphate-rich fluid |
Excellent — aqueous, room temp, no radicals |
Carboxylates protonated at gastric pH; Ca²⁺ displaced by phosphate at intestinal pH |
|
Polyelectrolyte complex |
Alginate–chitosan ionic pairing |
Good; reinforced by LBL deposition |
Excellent — no chemical reagents; aqueous mixing |
Anionic component swells as pH rises above pKa; erosion above pH 7.0 |
|
Covalent radical (permanent) |
MBA or EGDMA + AAm/AAc |
High; hydrolytically stable |
Moderate — radical intermediates risk Met/Trp oxidation; post-gelation loading needed |
Ionisable carboxylates swell mesh above pKa; macromolecular diffusion enabled at colonic pH |
|
Dynamic covalent Schiff base |
Oxidised CMC + chitosan amine |
Moderate; pH-labile below pH 5 |
Good — gelation at physiological pH/temp; self-healing; injectable |
Imine bonds hydrolyse at acidic pH; reform at neutral pH; net release by GI pH cycling |
|
Boronate ester (pH + ROS) |
Phenylboronic acid + cis-diol polymer |
Moderate; dual trigger required |
Good — aqueous crosslinking; dissolves only when both pH and ROS thresholds exceeded |
Boronate ester hydrolysed by acidic pH or H₂O₂; dual-trigger maximises colon specificity |
|
Photocrosslinking (UV) |
Methacrylated HA/GelMA + photoinitiator |
High; stable under GI conditions |
Moderate — low initiator conc limits radical exposure; far-UV risks nucleic acid damage |
Ionisable groups swell at colonic pH; crosslink density tuneable by irradiation dose |
Physical crosslinks — ionotropic Ca²⁺ coordination, polyelectrolyte pairing, hydrogen bonding — are inherently reversible and pH-sensitive. Boronate ester crosslinks are particularly attractive for dual-responsive colon targeting because they are hydrolysed by both acidic pH and H₂O₂, enabling disease-selective release in IBD tissue characterised by both near-neutral pH and elevated ROS.
5.2 Biologic Loading and Multilayer Architecture
Biologic loading strategy must be matched to molecular weight, charge, and conformational sensitivity of the payload. Table 4 compares fabrication methods and their biologic compatibility.
Table 4. Fabrication methods for pH-responsive hydrogels and their suitability for encapsulating macromolecular biologics.
|
Method |
Compatible Polymers |
Size Range |
Biologic Compatibility Considerations |
|
Ionotropic gelation |
Alginate, pectin, carrageenan |
500 µm–3 mm |
Excellent: aqueous, mild Ca²⁺ crosslinking at room temp; no radicals; widely used for proteins and antibodies |
|
Electrospray / coaxial |
Alginate, chitosan, PVA blends |
200 nm–500 µm |
Good: tunable size; coaxial configuration isolates biologic core from polymer shell minimising denaturation |
|
Free radical polymerisation |
PAA, Carbopol, IAc-AAm |
10 nm–1 µm |
Moderate: radical species risk protein oxidation; post-gelation loading with radical scavengers recommended |
|
Layer-by-layer (LBL) |
Alginate/chitosan + Eudragit coat |
1–10 µm |
Good: stepwise aqueous deposition; pH threshold tuneable by L100:S100 ratio; validated for protein-loaded beads |
|
Schiff base gelation |
Oxidised CMC + modified chitosan |
Injectable bulk gel |
Good: gelation within 30–120 s at physiological temperature; self-healing; no external crosslinker required |
|
Nanoparticle-in-hydrogel |
Alginate/HA + LNP/MOF/PLGA NPs |
Macrogel + 50–500 nm NPs |
Excellent for RNA: dual protection — NP shields siRNA/mRNA from nucleases; hydrogel absorbs acid and mechanical stress |
|
Spray-freeze-drying |
Eudragit, HPMC, alginate matrices |
1–200 µm |
Moderate-good: sub-ambient processing avoids heat denaturation; lyoprotectant selection critical; preferred over spray-drying for biologics |
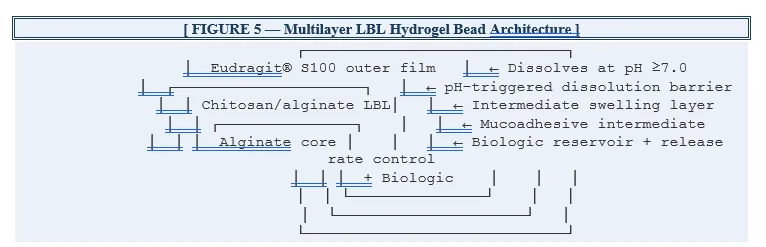
Figure 5. Cross-sectional schematic of a multilayer layer-by-layer (LBL) hydrogel bead for colon-targeted biologic delivery. The innermost alginate core serves as the biologic reservoir and primary release-rate-control domain; mesh size at gastric pH prevents biologic diffusion while swelling at colonic pH enables release. The intermediate chitosan/alginate LBL bilayers (typically 3–10 bilayers) provide additional mechanical stability, mucoadhesive surface charge, and microbiota enzyme-triggered degradability. The outermost Eudragit® S100 film ensures no payload liberation occurs before pH 7.0 is reached at the ileocaecal junction. Each functional layer is independently optimisable — a key advantage of LBL architecture over single-polymer systems.

Figure 6. Sequential protection architecture of the alginate–ZIF-8 MOF nanoparticle composite for oral siRNA delivery to the colon. ZIF-8 (zeolitic imidazolate framework-8) is a metal-organic framework formed by zinc ions coordinating with 2-methylimidazolate linkers, producing a crystalline porous structure with pore apertures of approximately 3.4 Å — small enough to exclude RNase A (hydrodynamic radius ~19 Å) while accommodating siRNA condensation through electrostatic interaction with zinc nodes. The surrounding sodium alginate hydrogel matrix provides acid stability at gastric pH through compact network maintenance and absorbs mechanical GI transit forces. At colonic pH, alginate swells and releases MOF nanoparticles, which are internalised by mucosal macrophages through endocytosis, with subsequent endosomal escape enabling cytoplasmic siRNA delivery and RISC-mediated mRNA silencing.
6. Recent Advances by Biologic Class
Table 3 consolidates recent documented outcomes for pH-responsive hydrogel systems evaluated for specific biologic payloads.
Table 3. Selected recent reports of pH-responsive hydrogel systems evaluated for colon-targeted biologic delivery.
|
Biologic Class |
Specific Agent |
Hydrogel Platform |
Reported Findings |
Experimental Model |
Ref. |
|
Anti-TNF-α mAb |
Infliximab analogue |
Folic acid-chitosan clay nanocomposite + pH coat |
Preserved IgG structure at pH 1.2 & 6.8; targeted delivery to folate receptor+ macrophages |
Caco-2; rat colitis |
[17] |
|
Anti-IL-6 mAb |
Recombinant anti-IL-6 |
Amino acid excipient core + pH/enzyme Eudragit coat |
Colonic tissue antibody uptake exceeded i.p. injection; IL-6 mRNA downregulation |
DSS colitis mouse |
[5] |
|
TNF-α Ab + MSC exosomes |
Anti-TNF IgG; UMSC-EXOs |
Fluidic microgel assembly (FMGA) |
48-h mucosal retention; ZO-1/occludin restoration; microbiota diversity recovered |
DSS mouse + beagle IBD |
[16] |
|
Model protein |
BSA (66 kDa) |
Alginate/chitosan nanospheres |
pH-dependent release; EE >80%; low haemolysis; low Caco-2 cytotoxicity |
In vitro |
[6] |
|
siRNA (gene silencing) |
TNF-α siRNA |
Sodium alginate + ZIF-8 MOF-siRNA nanoparticles |
Survived gastric acid; colonic accumulation; TNF-α knockdown; colitis amelioration |
DSS colitis mouse |
[21] |
|
siRNA (sustained) |
GFP-targeting siRNA |
Gellan gum + DOTAP lipoplexes |
60-day controlled release; retained knockdown in DLD1 colon cancer cells |
DLD1 CRC in vitro |
[22] |
|
ROS-scavenging nanogel |
IAc-AAm nanogel |
Itaconic acid–acrylamide nanogel (190 nm) |
10-fold swelling pH 1.2→7.4; superoxide scavenging 5× control; cytocompatible |
In vitro pH + ROS assays |
[3] |
6.1 Monoclonal Antibodies
Encapsulating anti-IL-6 antibodies in amino acid excipient cores surrounded by Eudragit® coating dissolving at colonic pH demonstrated that colonic tissue antibody concentrations after oral administration exceeded those from intraperitoneal injection at equivalent doses in DSS-induced colitis mice — with correspondingly greater IL-6 mRNA downregulation. Folic acid-grafted clay-chitosan nanocomposites loaded with an infliximab analogue confirmed intact antibody secondary and tertiary structure (CD spectroscopy, SDS-PAGE) after 2-hour simulated gastric exposure and site-selective delivery to folate receptor-expressing macrophages in inflamed colonic mucosa.
6.2 Therapeutic Proteins
Recombinant proteins including BSA (66 kDa), intestinal trefoil factor, and epidermal growth factor have been evaluated in pH-responsive systems with consistent documentation of pH-dependent release favouring liberation at colonic pH. An oral hydrogel nanoemulsion co-delivery system combining alginate/hyaluronic acid matrix achieved biphasic release — immediate burst from nanoemulsion droplets followed by sustained matrix release — with significant anti-inflammatory and barrier restoration outcomes in DSS-colitis models. The HA component provided CD44-mediated macrophage targeting, concentrating the anti-inflammatory payload in the innate immune cells primarily responsible for cytokine-driven mucosal damage.
6.3 siRNA and Exosomes
The alginate–ZIF-8 MOF composite (detailed in Figure 6) achieved survival of gastric acid, preferential colonic accumulation exploiting IBD-enhanced mucosal permeability, significant TNF-α mRNA knockdown, and histopathological colitis improvement. MSC-derived exosomes loaded into fluidic microgel assemblies (FMGAs) achieved 48-hour mucosal retention, restoration of ZO-1, occludin, and claudin-1 tight junction protein expression, and improved gut microbiota diversity in both DSS mouse colitis and a beagle canine IBD model.
7. Emerging Multi-Stimuli Responsive Systems
7.1 Dual pH/ROS Platforms
The pathological co-occurrence of near-neutral pH and markedly elevated ROS in actively inflamed colonic mucosa defines a two-variable signature enabling higher targeting specificity than either trigger independently. Mechanistically, ROS-responsive chemical linkages are incorporated into the hydrogel network alongside ionisable groups: thioketal bonds are cleaved by H₂O₂ through a peroxide-mediated hydrolysis mechanism; phenylboronate esters are oxidised by H₂O₂ to release phenol and borate; and ferrocene moieties cycle between Fe²⁺ and Fe³⁺ oxidation states in response to superoxide. Itaconic acid-acrylamide nanogels achieve dual-trigger functionality intrinsically: the carboxylic acid groups provide pH-triggered swelling (10-fold between gastric and colonic pH) while electron-rich vinyl and enone moieties in the IAc backbone scavenge superoxide through radical addition reactions — providing a ROS-scavenging activity five times greater than control formulations.

Figure 7. Mechanistic schematic of dual pH/ROS-responsive drug release in the IBD colonic microenvironment. In healthy colonic tissue, luminal pH is near-neutral (~7.2) and ROS concentrations are low — while pH may trigger partial ionisation, insufficient ROS prevents complete crosslink cleavage, maintaining network integrity. In actively inflamed IBD mucosa, both near-neutral pH (generating R-COO⁻ ionisation-driven swelling) and elevated H₂O₂ (cleaving thioketal or phenylboronate ester crosslinks) occur simultaneously, providing the dual trigger for network disintegration and biologic payload release specifically at the disease site. This pathology-selectivity principle improves the therapeutic index by preventing biologic release in non-inflamed colonic segments — a clinical advantage when limiting systemic biologic exposure is therapeutically important.
7.2 Enzyme-Responsive and AI-Assisted Design
Combining pH-triggered outer coating dissolution with enzymatic inner matrix degradation by colonic polysaccharidases creates systems requiring two simultaneous colonic conditions for release. The reliance on microbial enzymatic activity adds a disease-relevant adaptive dimension — dysbiotic IBD microbiota modulates enzyme availability, creating a pharmacokinetic profile that intensifies delivery as disease activity increases and enzyme diversity is restored. Machine learning QSPR models trained on polymer swelling datasets enable in silico prediction of swelling ratios for novel monomer combinations. Molecular dynamics simulations reveal that network heterogeneity rather than average mesh size is the dominant predictor of antibody diffusivity — a mechanistically important finding with direct crosslink density optimisation implications.
8. Characterisation Methodologies
Table 7 organises principal characterisation techniques, their outputs, and their significance for biologic hydrogel performance assessment.
Table 7. Characterisation methods for pH-responsive hydrogels loaded with biologic payloads.
|
Parameter |
Technique(s) |
Key Metrics |
Significance for Biologic Hydrogel |
|
pH-swelling response |
Gravimetric swelling at pH 1.2, 4.5, 6.8, 7.4 / 37°C |
ESR; swelling kinetics; transition threshold |
Primary functional descriptor; ESR fold-change pH 7.4 vs 1.2 defines colon selectivity |
|
Viscoelastic properties |
Dynamic oscillatory rheology |
G', G'', gel point, shear-recovery kinetics |
Confirms solid-like behaviour; G' predicts resistance to peristaltic disruption |
|
Chemical structure |
FTIR-ATR; ¹H NMR |
Crosslink bond formation; polymer–drug H-bonding; residual monomer |
Confirms crosslinking chemistry; reveals drug–polymer interaction; detects cytotoxic residuals |
|
Crystallinity / thermal |
XRD; DSC; TGA |
Crystallinity index; Tg, Tm; degradation onset |
Biologic amorphisation on encapsulation may alter stability; DSC Tm signals protein conformational state |
|
Particle morphology |
SEM (cryo-stage); AFM |
Pore size; homogeneity; bead sphericity |
Pore size vs biologic hydrodynamic radius governs diffusional release; cryo-SEM preserves swollen architecture |
|
Particle size and charge |
DLS; laser diffraction; zeta potential |
Z-average diameter; PDI; ζ-potential at different pH |
Size predicts mucosal penetration; pH-dependent size change confirms swelling |
|
Biologic secondary structure |
Far-UV CD; FTIR amide I/II |
α-helix %; β-sheet %; random coil |
Loss of α-helix or β-sheet indicates destabilisation affecting bioactivity |
|
Biologic tertiary structure |
Near-UV CD; Trp fluorescence; nanoDSF |
Aromatic microenvironment; Tm; ΔTm vs reference |
CDRs of antibodies reside in tertiary structure; Tm reduction >2°C signals relevant destabilisation |
|
Aggregation state |
SEC-MALS; SDS-PAGE non-reducing |
Monomer fraction %; HMW aggregate content |
Aggregates immunogenic and inactive; non-reducing SDS-PAGE reveals disulfide-bonded aggregates |
|
In vitro drug release |
USP Apparatus I/II; sequential pH change; biorelevant fluids |
Cumulative release (%); rate constant; kinetic model n-value |
Validates GI protection and colonic triggering; n-value from Korsmeyer-Peppas identifies diffusion vs swelling mechanism |
The Korsmeyer-Peppas n-value obtained from in vitro release data provides mechanistic insight into whether diffusion or swelling dominates release — critical for selecting formulation optimisation strategy. An n-value below 0.45 suggests Fickian diffusion and indicates crosslink density can be reduced to accelerate release at colonic pH. An n-value approaching 0.89 suggests swelling-rate control and indicates that polymer hydration rate — governed by network ionisation kinetics — is the bottleneck. The nanoDSF thermal stability measurement (Tm) serves as an early warning indicator of biologic destabilisation during formulation: a Tm reduction greater than 2°C relative to the free protein benchmark signals clinically relevant conformational perturbation requiring reformulation.
9. Translational Challenges
Table 5 organises principal translational obstacles, their mechanistic root causes, and current or emerging countermeasures.
Table 5. Principal translational challenges in developing pH-responsive hydrogels for oral biologic delivery, with proposed solutions.
|
Translational Challenge |
Mechanistic Root Cause |
Current / Emerging Countermeasures |
|
Acid-mediated biologic denaturation |
Gastric pH 1.2–2.0 unfolds protein tertiary structure; RNA hydrolyses within seconds |
Eudragit S100 outer coat; compact anionic network at gastric pH; amino acid excipient stabilisers; nanoparticle inner core |
|
Luminal protease attack |
Pepsin, trypsin, chymotrypsin, elastase and brush-border peptidases sequentially degrade protein and RNA |
Dense hydrogel mesh steric exclusion; co-encapsulated protease inhibitors; PEGylation; MOF cage for siRNA |
|
Premature small intestinal release |
PAA swells above pH 4.5; alginate dissolves in phosphate-rich intestinal fluid |
LBL multilayer with Eudragit S100 outer coat; higher-threshold synthetic copolymers |
|
Short colonic mucosal contact |
Peristalsis sweeps formulation past mucosa before adequate drug permeation |
Thiolated chitosan mucoadhesion; FMGA (48-h retention); CD44-targeted HA; carbopol-chitosan coatings |
|
Epithelial permeability barrier |
Tight junctions restrict paracellular transport >~1 nm hydrodynamic radius |
Chitosan tight junction opening; FcRn-mediated IgG transcytosis; CD44-mediated HA uptake |
|
Natural polymer batch variability |
Alginate M/G ratio, chitosan deacetylation, pectin esterification vary between batches |
Tight supplier CoA specifications; in-process QC; shift to semi-synthetic analogues |
|
Biologic stability during manufacture |
Radicals oxidise amino acid residues; agitation aggregates proteins; heat unfolds domains |
Post-gelation loading; trehalose/sucrose lyoprotectants; spray-freeze-drying; mild crosslinking |
|
Regulatory / IVIVC complexity |
Combination drug-device classification; no validated IVIVC for biologic hydrogels |
Early pre-submission meetings; biorelevant dissolution media; mechanistic PK modelling |
Biologic stability across the complete product lifecycle constitutes the most pervasive challenge. The Henderson-Hasselbalch equation explains why a biologic protein with a pI (isoelectric point) of 7.0 — near-neutral — is particularly vulnerable to aggregation during lyophilisation of an alginate matrix, as freeze-concentration effects raise local protein concentration while the amorphous polysaccharide matrix provides insufficient hydrogen-bonding stabilisation. Trehalose (0.5–1.0 M) and sucrose (0.2–0.5 M) act as preferential hydration agents — their hydroxyl groups preferentially interact with protein surfaces through water-replacement and water-structuring mechanisms, maintaining protein conformation during ice formation. Regulatory classification of combination drug-hydrogel products and the absence of validated IVIVC frameworks remain the most significant non-technical barriers.
10. Clinical Translation Landscape
10.1 Current Clinical Evidence
Table 8 consolidates available clinical and late-preclinical evidence.
Table 8. Clinical-stage and advanced preclinical oral biologic delivery platforms relevant to colon-targeted pH-responsive hydrogel development.
|
Product / Platform |
Biologic Type |
Delivery Technology |
Clinical Stage & Key Findings |
Indication |
Ref. |
|
AVX-470 (Avaxia) |
Bovine polyclonal anti-TNF-α IgG |
Uncoated oral capsule |
Phase IIa: tolerated to 3.5 g/day; faecal anti-TNF activity; mucosal healing signals |
Ulcerative colitis |
[26] |
|
OPRX-106 (Protalix) |
Recombinant anti-TNF fusion protein |
Plant cell matrix; pH-sensitive release |
Phase II: dose-dependent clinical response; detectable faecal drug concentrations |
Ulcerative colitis |
[5] |
|
ORA-101 (research) |
Anti-IL-6 antibody |
pH/enzyme dual-sensitive Eudragit + amino acid core |
Preclinical: superior mucosal delivery vs i.p. injection in DSS mouse; Phase I planned |
Crohn's / UC |
[5] |
|
CALY-002 (siRNA) |
siRNA targeting STAT3 / TL1A |
LNP; oral LNP-hydrogel composite in development |
Phase IIa (subcutaneous); oral hydrogel composite in early preclinical stage |
IBD / CRC |
[23] |
|
FMGA exosome (academic) |
MSC-derived exosomes (UMSC-EXO) |
Fluidic microgel assembly (FMGA) |
Preclinical: 48-h colonic retention; tight junction restoration in mouse and beagle models |
IBD |
[16] |
|
Tamarind gum hydrogel (academic) |
Model protein / anti-inflammatory cargo |
β-CD-g-PMAA / tamarind gum crosslinked hydrogel |
In vitro: <5% release pH 1.2; >94% at pH 7.4 over 30 h; biocompatible MTT assay |
Colon delivery |
[8] |
The AVX-470 programme established feasibility of oral antibody dosing in humans and confirmed biologically active antibody reaching the colonic lumen. OPRX-106's Phase II success demonstrated dose-dependent clinical response and detectable faecal drug concentrations — quantifying the performance gap that pH-responsive hydrogel technology must close. A 100-fold improvement in mucosal bioavailability through Eudragit S100 + alginate protection would reduce required doses from grams to tens of milligrams, transforming economic feasibility.
10.2 FUTURE DIRECTIONS
Future developments include real-time physiological sensing for patient-specific adaptive release, living therapeutic cell carriers within pH-responsive matrices for continuous local biologic production, organ-on-chip models for human-relevant preclinical evaluation, and pharmacoeconomic strategies exploiting the high annual costs (USD 20,000–50,000) of parenteral biologic IBD therapy as economic justification for oral alternative development.
CONCLUSIONS
pH-responsive hydrogels represent a mechanistically well-grounded and experimentally validated approach to oral colon-targeted biologic delivery. The Donnan osmotic swelling mechanism, Flory-Rehner network thermodynamics, mesh-size-controlled macromolecular diffusion, and Korsmeyer-Peppas kinetic modelling together provide a rigorous quantitative framework for understanding, designing, and optimising these systems at the M.Pharm level. Polymer chemistry has evolved from single-component alginate and Eudragit® systems to dual-functional itaconic acid nanogels with intrinsic ROS scavenging, dynamic covalent Schiff base hydrogels with injectable and self-healing properties, and nanoparticle-in-hydrogel composites providing two-layer RNA protection. Formulation architecture advances — LBL multilayer beads, FMGAs with 48-hour mucosal retention, siRNA-MOF-alginate composites — have delivered therapeutic efficacy for anti-TNF-α antibodies, siRNA, and MSC-derived exosomes in preclinical IBD models.
Ten summary tables and seven schematic figure descriptions in this review consolidate the mechanistic, physicochemical, clinical, and translational knowledge base of the field. The principal translational challenges — biologic stability, natural polymer variability, scale-up manufacturing, combination product regulatory complexity, and absence of validated IVIVC frameworks — require sustained interdisciplinary effort. With continued collaboration across polymer science, pharmaceutical engineering, mechanistic pharmacokinetics, clinical gastroenterology, and regulatory science, pH-responsive hydrogels hold genuine promise as enabling platforms for the next generation of oral biologic therapies for colonic disease.
REFERENCES
Donnan FG. The theory of membrane equilibria. Chemical Reviews. 1924;1(1):73–90



Gautami Gangurde, Dr. Anil Jadhav, Dr. Atul Bendale, Prajwal Aher, pH-Responsive Hydrogels for Oral Colon-Targeted Delivery of Biologics: Recent Advances, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 665-687, https://doi.org/10.5281/zenodo.21156827
 10.5281/zenodo.21156827
10.5281/zenodo.21156827