
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Dr. V.V Patil Foundation’s College of Pharmacy, Vilad Ghat, Ahilyanagar, Maharashtra, India, 414111.
Ocular diseases linked to oxidative stress and inflammation—such as dry eye, diabetic retinopathy, and age?related macular degeneration—remain challenging to treat because of the eye’s intricate structure and protective barriers. Traditional eye drops often fail to deliver meaningful benefits, as they are quickly washed away, penetrate poorly through the cornea, and achieve very low drug levels inside the eye. This greatly limits the therapeutic impact of antioxidants like quercetin and gallic acid.Solid lipid nanoparticles (SLNs) have emerged as a promising solution. Built from biocompatible lipids and designed at the nanoscale, they can improve drug stability, sustain release, and enhance penetration into ocular tissues. This review explores how SLNs and related lipid?based carriers can boost the delivery of quercetin and gallic acid. Both antioxidants are known for their strong free?radical scavenging, anti?inflammatory, and cell?protective properties, making them highly relevant to eye disease.Formulation factors—such as lipid type, surfactant choice, particle size, surface charge, entrapment efficiency, and crystalline structure—play a crucial role in determining how well these systems cross the cornea and preserve drug activity. Recent studies show that SLNs and nanostructured lipid carriers (NLCs) markedly improve solubility, guard against degradation, and increase corneal transport compared to simple drug solutions. Other approaches, like hot?melt films and chitosan nanoparticles, also offer benefits by prolonging drug contact with the ocular surface.Overall, SLNs represent a versatile and clinically relevant platform for delivering quercetin and gallic acid to both the front and back of the eye. With continued refinement—such as optimizing lipid blends, exploring dual?drug loading, and developing hybrid systems—these carriers could accelerate the translation of antioxidant?based therapies into effective treatments for chronic eye diseases.
Eye diseases are a major global health issue, affecting millions of people and causing significant visual impairment. Conditions such as dry eye disease, diabetic retinopathy, glaucoma, and age‑related macular degeneration are becoming more common, driven by aging populations, environmental pollution, prolonged screen use, and systemic illnesses like diabetes and hypertension. Beyond vision loss, these disorders reduce independence, productivity, and overall quality of life, while also placing a heavy economic burden on healthcare systems through direct medical costs, long‑term care, and lost productivity.
Although treatments exist, their effectiveness is often limited by the difficulty of delivering drugs to the eye. The eye’s protective anatomy and physiology make drug delivery uniquely challenging. Tear turnover, blinking, and drainage rapidly clear topical medications, while the corneal epithelium blocks hydrophilic molecules and the stroma restricts lipophilic ones. Blood–aqueous and blood–retinal barriers further prevent systemic drugs from reaching therapeutic levels inside the eye. As a result, conventional formulations like drops, suspensions, and ointments require frequent dosing yet still fail to maintain sustained drug concentrations.
Oxidative stress is a key driver of many ocular diseases. Constant exposure to UV light, high oxygen levels, and environmental pollutants generates reactive oxygen species (ROS), which damage lipids, proteins, and mitochondria, trigger inflammation, and ultimately lead to cell death and tissue degeneration. Natural antioxidants such as quercetin and gallic acid are of great interest because of their strong free‑radical scavenging, anti‑inflammatory, and protective effects. However, their clinical use is hampered by poor solubility, instability, and limited ability to cross ocular barriers.
Solid lipid nanoparticles (SLNs) offer a promising way forward. Their nanoscale size improves corneal penetration, while the lipid matrix enhances solubility and shields antioxidants from degradation. SLNs also extend drug residence time on the ocular surface and enable sustained release, reducing the need for frequent dosing and improving therapeutic outcomes. These features make SLNs an attractive platform for delivering quercetin and gallic acid, opening new possibilities for treating eye diseases driven by oxidative stress. [2,3]
Background of Disease and Drugs
1. Diabetic retinopathy
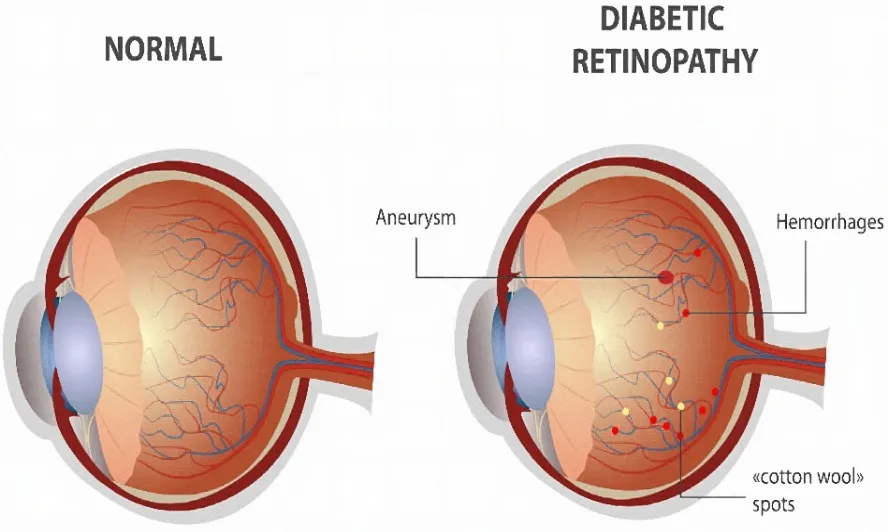
Fig.1. Diabetic Retinopathy
What It Is
Diabetic retinopathy is an eye condition that develops in people with diabetes. It happens when high blood sugar damages the tiny blood vessels in the retina—the part of the eye that senses light and helps us see clearly. If left untreated, it can gradually lead to serious vision problems and even blindness.
Why It Happens
When blood sugar stays too high for too long, it weakens the retinal blood vessels. These vessels may start leaking fluid or bleeding. In advanced stages, the body tries to grow new vessels, but they’re fragile and often break easily, making the problem worse.
Signs & Symptoms
• Early stage: Usually no noticeable symptoms.
• Later stage: Blurred vision, floating dark spots, trouble seeing at night, and eventually vision loss.
Types & Stages
1. Non-Proliferative Diabetic Retinopathy (NPDR)
• Early stage.
• Blood vessels leak or close off.
• Vision changes are usually mild at this point.
2. Proliferative Diabetic Retinopathy (PDR)
• Advanced stage.
• New, abnormal vessels grow but are fragile.
• Can cause bleeding inside the eye and severe vision loss.
Risk Factors
• Having diabetes for many years (type 1 or type 2).
• Poor blood sugar control.
• High blood pressure or cholesterol.
• Pregnancy in women with diabetes.
Prevention & Care
• Regular eye check-ups: Annual dilated eye exams are key to catching problems early.
• Healthy control: Keeping blood sugar, blood pressure, and cholesterol in range lowers risk.
• Treatment options: Depending on severity, doctors may recommend eye injections, laser therapy, or surgery to slow or stop progression.[4]
2. Age-related macular degeneration (AMD)
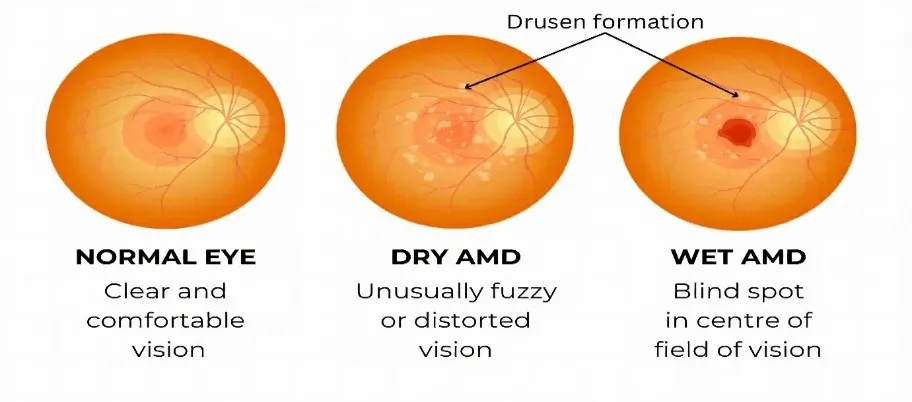
Fig. 2. Age-related macular degeneration (AMD)
What It Is
AMD is an eye disease that develops as we age, affecting the macula—the small but vital part of the retina that gives us sharp, central vision. When the macula deteriorates, everyday tasks like reading, driving, or recognizing faces become difficult. AMD is the leading cause of vision loss in people over 50, but it doesn’t affect side (peripheral) vision.
How It Affects Vision
People with AMD may notice:
• Blurry or wavy central vision
• Blank or dark spots in the middle of what they see
• Trouble seeing fine details
• Difficulty adjusting to dim light
Types of AMD
1. Dry AMD
• Most common (about 80–90% of cases).
• Caused by thinning of the macula and buildup of yellow deposits called drusen.
• Progresses slowly.
• Symptoms: blurred central vision, needing brighter light, difficulty recognizing faces.
2. Wet AMD
• Less common but more serious.
• Caused by abnormal blood vessels growing under the retina, which leak fluid or blood.
• Progresses quickly if untreated.
• Symptoms: distorted vision (straight lines look wavy), dark spots in central vision.
Risk Factors
• Age: Most common after 50.
• Genetics: Family history increases risk.
• Lifestyle: Smoking, poor diet, obesity, high blood pressure.
• Race: More common in Caucasians.
• Gender: Slightly higher in women.
Diagnosis
• Dilated eye exam: Doctors look for drusen and macular changes.
• Amsler grid test: Detects wavy or distorted vision.
• OCT scan: Provides detailed images of the retina.
Treatment & Management
• Dry AMD: No cure, but progression can be slowed with healthy lifestyle changes and AREDS2 supplements (vitamins and antioxidants).
• Wet AMD: Treated with anti-VEGF injections, photodynamic therapy, or laser surgery (less common today).
• Low vision aids: Magnifiers, special glasses, and adaptive devices help maximize remaining vision.
Prevention & Lifestyle Tips
• Quit smoking.
• Eat leafy greens, fish, and foods rich in antioxidants.
• Keep blood pressure and cholesterol under control.
• Protect eyes from UV light.
• Get regular eye exams after age 50. [5]
3.Glaucoma
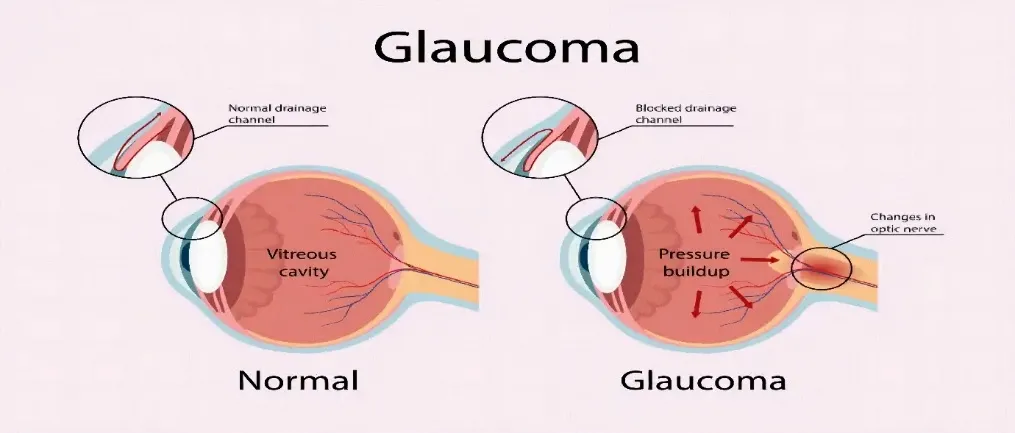
Fig. 3. Glaucoma
What It Is
Glaucoma is a group of eye diseases that damage the optic nerve—the “cable” that carries visual signals from your eye to your brain. This damage is often linked to fluid buildup in the eye that raises pressure, but glaucoma can also occur even when eye pressure is normal. It’s more common as we get older and is one of the leading causes of permanent blindness worldwide. The good news: with early detection and proper treatment, most vision loss can be prevented.
How It Affects Vision
• Optic nerve damage: Vision loss usually starts at the edges (peripheral vision) and slowly moves inward.
• Pressure mechanism: Normally, fluid inside the eye drains through a mesh-like channel. If drainage is blocked, pressure rises and harms the optic nerve.
• Normal-tension glaucoma: Some people develop glaucoma even with normal pressure, likely due to blood flow or nerve sensitivity.
Types of Glaucoma
1. Open-angle glaucoma
• Most common type.
• Drainage angle looks normal, but fluid doesn’t drain well.
• Progresses slowly and painlessly, often unnoticed until vision loss is significant.
2. Angle-closure glaucoma
• Drainage angle becomes blocked or narrowed.
• Can cause sudden, severe pressure rise (acute attack).
• Symptoms: intense eye pain, blurred vision, halos around lights, headache, nausea. This is a medical emergency.
3. Normal-tension glaucoma
• Optic nerve damage occurs despite normal pressure readings.
• Likely linked to circulation or nerve structure.
4. Secondary & congenital glaucoma
• Caused by other eye problems, injuries, medications (like steroids), or present from birth due to drainage system issues.
Symptoms & Warning Signs
• Open-angle: Gradual loss of side vision, trouble with contrast or dim light.
• Angle-closure (acute): Sudden severe eye pain, red eye, halos, headache, nausea/vomiting—urgent care needed.
• Normal-tension: Similar vision loss pattern, even with normal pressure.
Who Is at Risk
• Age over 60.
• Family history of glaucoma.
• Elevated eye pressure.
• Eye anatomy factors (thin corneas, narrow angles).
• Certain medications (especially steroids), past eye injuries, or vascular issues.
Diagnosis
• Comprehensive eye exam: Includes pressure check, drainage angle exam, optic nerve imaging, and visual field testing.
• Monitoring over time: Glaucoma is confirmed when both structural damage and functional vision loss are consistently observed.
Treatment Goals & Options
The aim is to preserve vision by slowing or stopping optic nerve damage, usually by lowering eye pressure.
• Eye drops: First-line treatment; reduce fluid production or improve drainage.
• Oral medications: Sometimes used short-term.
• Laser procedures: Improve fluid outflow or open blocked angles.
• Surgery: Options like trabeculectomy, drainage devices, or minimally invasive glaucoma surgery (MIGS).
Living With Glaucoma
• Regular check-ups: Stay consistent with exams and visual field tests.
• Stick to medications: Missing doses can let pressure rise and worsen damage.
• Know your numbers: Track your target eye pressure and typical readings.
• Support your health: Manage blood pressure and circulation, avoid smoking, and report side effects promptly. [6,7]
Drugs
1. Quercetin
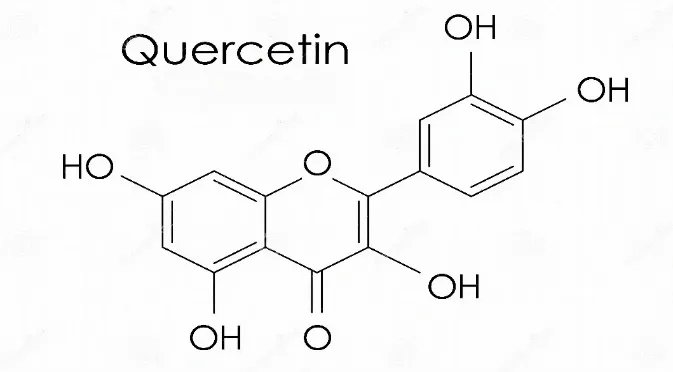
Fig. 4. Structure of Quercetin
What is Quercetin?
Quercetin is a natural compound (a flavonoid) found in foods like apples, onions, berries, and tea. It’s well known for its antioxidant power, helping to neutralize harmful free radicals and reduce oxidative stress. Beyond that, it also has anti-inflammatory, anti-carcinogenic, and anti-apoptotic (cell-protecting) effects, making it a promising candidate for treating eye diseases.
Challenges in Eye Delivery
Delivering drugs to the eye isn’t easy because:
• Tears and blinking quickly wash away medicines.
• The cornea acts as a strong barrier, limiting penetration.
• Quercetin itself has poor solubility, so it doesn’t dissolve well in eye drops.
Why Quercetin Matters in Eye Care
1. Therapeutic Benefits
• Antioxidant shield: Protects retinal cells from oxidative damage (important in AMD and cataracts).
• Anti-inflammatory: Reduces cytokine release, helping in uveitis and dry eye syndrome.
• Neuroprotection: Safeguards retinal ganglion cells, relevant in glaucoma.
2. Advanced Delivery Systems
• Microemulsions: Improve solubility and corneal penetration, with sustained release.
• Solid Lipid Nanoparticles (SLNs): Encapsulate quercetin for controlled release, safe and effective.
• Liposomes: Biocompatible carriers that enhance penetration and reduce irritation.
• Hydrogels: Provide longer retention on the eye surface for sustained action.
3. Clinical Applications
• Cataracts: Prevents lens protein oxidation.
• Glaucoma: Protects optic nerve cells from oxidative stress.
• Dry Eye Syndrome: Reduces inflammation and improves tear film stability.
• Corneal injuries: Promotes healing and reduces oxidative damage.
How Quercetin Works
• Antioxidant: Neutralizes reactive oxygen species (ROS) that damage lens proteins and retinal cells.
• Anti-inflammatory: Suppresses harmful cytokines like IL-1β and TNF-α.
• Anti-apoptotic: Prevents cell death in retinal and lens cells.
• Neuroprotective: Shields retinal neurons from oxidative and ischemic damage.
Quercetin in Specific Eye Diseases
• Cataracts: Delays progression by preventing protein oxidation and supporting lens cell survival.
• Glaucoma: Protects retinal ganglion cells, slowing optic nerve damage.
• AMD (Age-related Macular Degeneration): Reduces oxidative stress in retinal pigment cells, maintaining retinal health.
• Diabetic Retinopathy: Inhibits VEGF (a growth factor that drives abnormal vessel growth), reducing retinal damage.
• Dry Eye Syndrome: Lowers inflammation, stabilizes tear film, and eases discomfort.
• Corneal Injuries: Speeds healing and reduces oxidative stress. [8]
2. Gallic acid
Fig. 5. Structure of Gallic Acid
What is Gallic Acid?
Gallic acid (GA) is a natural compound found in foods like tea, grapes, berries, and gallnuts. It’s known for its antioxidant strength, along with anti-inflammatory, anti-apoptotic (cell-protecting), and even antimicrobial properties. In eye care, its antioxidant ability is especially important because oxidative stress is a major factor in many vision problems.
Challenges in Eye Delivery
Getting GA into the eye effectively is tricky because:
• It doesn’t dissolve well and has poor bioavailability.
• Tears and blinking quickly wash away medicines.
• The cornea acts as a strong barrier, limiting drug penetration.
Why Gallic Acid Matters in Eye Care
1. Therapeutic Benefits
• Antioxidant shield: Neutralizes harmful free radicals, protecting lens proteins and retinal cells.
• Anti-inflammatory: Suppresses cytokines that drive inflammation, useful in dry eye and uveitis.
• Anti-apoptotic: Prevents cell death in retinal ganglion and lens epithelial cells.
• Neuroprotection: Helps safeguard retinal neurons, relevant in glaucoma and diabetic retinopathy.
• Anti-angiogenic: Inhibits abnormal blood vessel growth, important in AMD and diabetic retinopathy.
2. Advanced Delivery Systems
• Nanoparticles: Encapsulate GA for controlled release, improving solubility and penetration.
• Liposomes: Biocompatible carriers that boost bioavailability and reduce irritation.
• Hydrogels: Provide sustained release on the eye surface, increasing retention time.
• Microemulsions: Enhance solubility and stability for better therapeutic effect.
3. Applications in Eye Diseases
• Cataracts: Prevents oxidative damage to lens proteins, slowing progression.
• Glaucoma: Protects optic nerve cells from oxidative stress and apoptosis.
• AMD (Age-related Macular Degeneration): Reduces oxidative damage in retinal pigment cells.
• Diabetic Retinopathy: Inhibits VEGF and oxidative stress, reducing abnormal vessel growth.
• Dry Eye Syndrome: Lowers inflammation and oxidative damage, improving tear film stability.
• Corneal Injuries: Promotes healing and reduces oxidative stress.
How Gallic Acid Works
• Antioxidant: Scavenges reactive oxygen species (ROS).
• Anti-inflammatory: Suppresses cytokines like TNF-α and IL-1β.
• Anti-apoptotic: Prevents programmed cell death in key eye cells.
• Neuroprotective: Shields retinal neurons from oxidative and ischemic damage.
• Anti-angiogenic: Blocks abnormal blood vessel formation. [9,10]
2. SOLID LIPID NANOPARTICLES & NANOSTRUCTURED LIPID CARRIERS
Solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs) are advanced lipid‑based systems designed to address the shortcomings of conventional eye formulations. Their biocompatibility, nanoscale size, and ability to encapsulate poorly soluble molecules make them especially promising for delivering antioxidants like quercetin and gallic acid to ocular tissues.
Composition and Preparation
SLNs are built entirely from solid lipids that remain stable at both room and body temperature. Common choices include glyceryl monostearate, Compritol 888 ATO, stearic acid, and Precirol ATO. These lipids form a rigid crystalline matrix that can trap hydrophobic drugs. NLCs, on the other hand, combine solid and liquid lipids (such as Miglyol 812 or oleic acid), producing a less ordered structure that allows for higher drug loading and reduces the risk of drug expulsion during storage. Surfactants like Tween 80, Poloxamer 188, or lecithin are added to stabilize the dispersion.
Several methods are used to prepare these carriers. High‑pressure homogenization is the most common because it is scalable and avoids organic solvents. In hot homogenization, the drug is dissolved in melted lipid and emulsified into a heated surfactant solution before homogenization and cooling. Cold homogenization is better suited for heat‑sensitive drugs. Other techniques—such as ultrasonication, microemulsion dilution, solvent emulsification–evaporation, and solvent injection—offer flexibility depending on the drug’s properties and formulation goals.
Physicochemical Characterization
Thorough characterization ensures stability, safety, and therapeutic effectiveness. Particle sizes usually fall between 50–200 nm, which supports corneal penetration. A polydispersity index (PDI) below 0.3 indicates uniformity and stability. Zeta potential values above ±20 mV help prevent aggregation, while positively charged particles adhere more effectively to the negatively charged corneal surface. Entrapment efficiency is typically high—often above 80%—with NLCs achieving even greater values thanks to their disordered matrix. Other important parameters include morphology (via TEM/SEM), crystallinity (DSC/XRD), pH, osmolarity, viscosity, and drug release profiles.
Advantages Over Conventional Systems
Compared to traditional eye drops and suspensions, SLNs and NLCs offer clear benefits. Their nanoscale size improves corneal penetration, while their lipid composition enhances solubility and protects sensitive drugs from degradation. They also extend drug residence time on the ocular surface, reducing losses from tear turnover and drainage. Sustained release reduces dosing frequency, improving patient compliance. Their compatibility with hydrophobic antioxidants makes them particularly well‑suited for treating oxidative stress‑related eye diseases.
SLNs vs. NLCs
Although both systems share many features, their differences affect performance. SLNs have a highly crystalline matrix that supports controlled release but limits drug loading and may cause drug expulsion during storage. NLCs, by incorporating liquid lipids, create structural imperfections that improve drug loading, stability, and release flexibility. NLCs often show smaller particle sizes, lower PDI values, and better long‑term stability. SLNs are best suited for applications requiring slow, controlled release, while NLCs are preferred when higher drug loading and enhanced stability are needed. [11,12]
3. QUERCETIN IN OPHTHALMIC DELIVERY
Quercetin is a plant‑derived flavonoid best known for its powerful antioxidant, anti‑inflammatory, and neuroprotective effects. These properties make it an attractive candidate for treating eye diseases linked to oxidative stress and inflammation, such as dry eye, diabetic retinopathy, glaucoma, and age‑related macular degeneration. Yet, despite its promise, quercetin’s clinical use in ophthalmology has been hampered by poor water solubility, rapid breakdown, and low bioavailability in ocular tissues—challenges that highlight the need for advanced delivery systems like SLNs, NLCs, and polymeric nanoparticles.
Pharmacological Profile
Quercetin’s antioxidant strength comes from its polyphenolic structure, which allows it to neutralize reactive oxygen species (ROS), prevent lipid peroxidation, and protect mitochondrial function. These actions are particularly important in the eye, where oxidative stress contributes to corneal damage, retinal degeneration, and dysfunction of the trabecular meshwork.
Its anti‑inflammatory activity is linked to the suppression of pathways such as NF‑κB, COX, and LOX. By downregulating pro‑inflammatory cytokines like IL‑6, TNF‑α, and IL‑1β, quercetin helps reduce ocular surface inflammation and retinal injury. In addition, its neuroprotective effects safeguard retinal ganglion cells and photoreceptors by stabilizing mitochondria, lowering caspase activation, and regulating calcium balance. Together, these mechanisms position quercetin as a versatile therapeutic agent for both anterior and posterior eye disorders.
Challenges in Ocular Delivery
Despite these benefits, quercetin faces significant delivery hurdles. Its poor solubility in water, instability in aqueous environments, and limited ability to cross the corneal epithelium mean that conventional eye drops cannot achieve therapeutic concentrations. Rapid clearance from the ocular surface further reduces bioavailability, underscoring the importance of nanocarrier systems that can improve solubility, protect against degradation, and enhance penetration.
Evidence from Recent Studies
• Truong (2017): SLNs, NLCs, and Hot‑Melt Films
Truong compared quercetin‑loaded SLNs, NLCs, and hot‑melt films. While SLNs and NLCs showed good physicochemical properties—with NLCs offering higher entrapment efficiency and smaller particle size—the hot‑melt films achieved the highest corneal permeability, nearly four times greater than the nanoparticles. This was attributed to longer contact with the ocular surface and higher local drug concentration. The study confirmed that lipid‑based nanoparticles improve quercetin delivery, but film‑based systems may provide superior penetration.
• Eltanameli (2021): Chitosan Nanoparticles for Dry Eye
Eltanameli developed quercetin‑loaded chitosan nanoparticles using ionic gelation. These carriers significantly enhanced solubility and sustained drug release for up to 96 hours. Their positive surface charge improved adhesion and uptake by the cornea. Importantly, they reduced IL‑6 expression by over 36%, demonstrating strong anti‑inflammatory activity. This work highlights the promise of polymeric nanoparticles for treating ocular surface conditions such as dry eye disease. [14]
4. GALLIC ACID IN OPHTHALMIC DELIVERY
Gallic acid (GA) is a naturally occurring phenolic compound found in fruits, tea, and medicinal plants. In recent years, it has attracted growing interest in ophthalmic research thanks to its strong antioxidant, anti‑inflammatory, and protective properties. These actions make GA a promising candidate for treating ocular surface disorders such as dry eye disease (DED), where oxidative stress and inflammation are key drivers of pathology. Like many natural antioxidants, however, GA faces challenges with stability and ocular penetration, which has prompted the exploration of advanced carriers such as SLNs, NLCs, and polymeric nanoparticles.
Pharmacological Profile
GA’s antioxidant power comes from its three hydroxyl groups, which give it high electron‑donating capacity. This allows GA to quickly neutralize reactive oxygen species (ROS), inhibit lipid peroxidation, and chelate metal ions that fuel oxidative reactions. In the eye, these effects protect corneal epithelial cells, conjunctival goblet cells, and lacrimal glands from oxidative damage.
GA also exerts notable anti‑inflammatory effects by suppressing cytokines such as IL‑6, TNF‑α, and IL‑1β, which are elevated in DED and contribute to epithelial injury and tear film instability. In addition, GA reduces caspase activation, helping prevent apoptosis in stressed ocular cells. Together, these mechanisms make GA a strong candidate for managing oxidative and inflammatory eye conditions.
Evidence from Li et al. (2023)
Li and colleagues provided both in vitro and in vivo evidence of GA’s therapeutic potential in dry eye disease. In cell culture studies, GA lowered ROS levels in human corneal epithelial cells exposed to hyperosmotic stress—a hallmark of DED. It also suppressed inflammatory signalling in macrophages, showing its ability to modulate immune responses relevant to ocular surface inflammation.
In mouse models, topical GA improved tear secretion, restored goblet cell density, and reduced corneal epithelial apoptosis. Tissue analysis revealed less inflammatory infiltration and better epithelial integrity. These findings confirm GA’s multi‑level protective role against the mechanisms driving dry eye disease.
Mechanistic Insights
Two key molecular pathways explain GA’s effects:
1. NF‑κB Inhibition – GA blocks NF‑κB activation, reducing the expression of inflammatory mediators such as IL‑6, TNF‑α, and MMP‑9.
2. Nrf2 Activation – GA stimulates Nrf2 signalling, which boosts antioxidant enzymes like HO‑1, SOD, and catalase, strengthening cellular defences against oxidative stress.
Potential Synergy with Quercetin
GA and quercetin complement each other in ways that make them ideal for combination therapy:
• Both neutralize ROS, but quercetin stabilizes mitochondria while GA activates Nrf2.
• Both inhibit NF‑κB, reducing inflammatory cytokine production.
• GA is water‑soluble, while quercetin is lipophilic—together they span a wider solubility range.
• Dual‑loaded SLNs or NLCs could harness these complementary mechanisms, offering enhanced antioxidant and anti‑inflammatory protection.
This synergy suggests that co‑delivery of GA and quercetin in lipid nanoparticles could provide superior outcomes for eye diseases driven by oxidative stress and inflammation. [15,16]
5. FORMULATION STRATEGIES FOR SLNS WITH QUERCETIN & GALLIC ACID
Designing solid lipid nanoparticles (SLNs) for the delivery of quercetin and gallic acid to the eye requires thoughtful selection of lipids, surfactants, and strategies to improve solubility. Quercetin is highly lipophilic and poorly soluble in water, while gallic acid is more hydrophilic but prone to instability in aqueous environments. SLNs provide a flexible platform that can encapsulate both molecules, shield them from degradation, and enhance their penetration into ocular tissues.
Lipid Excipients: Compritol, GMS, and Miglyol
The lipid matrix forms the backbone of SLN formulations. Compritol 888 ATO (glyceryl behenate) is a popular choice because of its high melting point, biocompatibility, and ability to create a stable crystalline structure. This matrix not only protects sensitive antioxidants but also supports sustained drug release.
Glyceryl monostearate (GMS) is another widely used lipid. Its amphiphilic nature improves solubilization of quercetin and contributes to smaller particle sizes, which are advantageous for ocular penetration.
Although SLNs traditionally rely solely on solid lipids, incorporating small amounts of Miglyol 812 (a medium‑chain triglyceride) can reduce crystallinity and improve drug loading. This hybrid approach creates a structure closer to nanostructured lipid carriers (NLCs), making it particularly useful for dual‑loaded systems that combine quercetin and gallic acid. [17,18]
Surfactants: Tween 80 and Poloxamer
Surfactants are essential for stabilizing SLNs and preventing particle aggregation. Tween 80 is widely used in ocular formulations because of its excellent biocompatibility, ability to lower interfacial tension, and capacity to enhance corneal permeability by loosening tight junctions in the epithelium. Poloxamer 188, a non‑ionic block copolymer, provides steric stabilization and helps achieve uniform particle sizes. When used together, Tween 80 and Poloxamer often produce smaller particles, lower polydispersity, and higher entrapment efficiency for drugs like quercetin and gallic acid.
Cyclodextrin Inclusion Complexes for Solubility Enhancement
Cyclodextrins (CDs) are valuable excipients for improving solubility and stability of poorly water‑soluble drugs. Forming quercetin–cyclodextrin inclusion complexes before incorporating them into SLNs enhances drug loading and prevents crystallization during storage. Hydroxypropyl‑β‑cyclodextrin (HPβCD) is especially effective due to its high solubility and established safety in ophthalmic use. For gallic acid, CDs help stabilize the molecule against oxidation and improve compatibility with the lipid matrix. Incorporating CD complexes into SLNs creates a dual‑level solubility enhancement system, improving both encapsulation and release behaviour.
Combination Therapy: Dual‑Loaded SLNs (Quercetin + Gallic Acid)
Co‑encapsulating quercetin and gallic acid in a single SLN system offers synergistic therapeutic benefits. Quercetin protects mitochondria and reduces inflammation, while gallic acid activates Nrf2 and suppresses NF‑κB signalling. Together, they provide complementary antioxidant and anti‑inflammatory effects. Dual‑loaded SLNs shield both molecules from degradation and ensure sustained release, prolonging therapeutic action on the ocular surface.
Hot‑Melt Cast Films vs. SLNs: Comparative Advantages
Hot‑melt cast films, as shown in Truong’s study, achieve superior corneal permeability because they remain in contact with the ocular surface longer and deliver higher local drug concentrations. They are simple to manufacture and provide excellent retention. However, films may cause discomfort, dissolve slowly, and are less effective for reaching posterior eye tissues. SLNs, in contrast, are more comfortable for patients, penetrate deeper into ocular tissues, and are suitable for both anterior and posterior delivery. They also offer controlled release, improved stability, and the ability to carry dual‑drug combinations—advantages that films cannot fully match. [19,20]
6. PRECLINICAL & CLINICAL EVIDENCE
Preclinical research has been crucial in uncovering how quercetin‑ and gallic acid‑loaded solid lipid nanoparticles (SLNs) and related nanocarriers behave in the eye. These studies—ranging from cell‑based assays to animal models and ex vivo corneal permeability experiments—consistently show that antioxidant‑loaded SLNs hold strong promise for treating ocular diseases. Still, despite encouraging findings, several hurdles remain before these systems can be fully translated into clinical use.
Rabbit Corneal Permeability Studies
Rabbit corneal models are commonly employed because their anatomy closely resembles that of the human cornea. Investigations using quercetin‑loaded SLNs and NLCs have demonstrated markedly improved permeability compared to free drug solutions. Truong’s study, for example, showed that both SLNs and NLCs enhanced quercetin transport across excised rabbit corneas, while hot‑melt cast films achieved the highest flux. This superior performance was attributed to longer contact with the ocular surface and higher local drug concentrations.
These results highlight the ability of lipid nanoparticles to overcome the corneal epithelial barrier—a major limitation of conventional eye drops. For gallic acid, SLN formulations similarly improved penetration by boosting solubility and protecting the compound from rapid breakdown in tear fluid. [21,22]
Mouse Dry Eye Models
Mouse models of dry eye disease (DED) provide valuable in vivo evidence of therapeutic potential. In 2023, Li and colleagues showed that topical gallic acid improved tear secretion, restored goblet cell density, and reduced corneal epithelial cell death in hyperosmolarity‑induced DED. These protective effects were linked to GA’s ability to block NF‑κB‑driven inflammation while activating Nrf2‑mediated antioxidant pathways. Although quercetin has been studied less extensively in vivo, available data suggest that quercetin‑loaded nanoparticles reduce oxidative stress, suppress inflammatory cytokines, and protect ocular surface tissues. SLNs and NLCs further enhance drug retention on the eye’s surface, enabling sustained therapeutic activity in DED models.
Cell Line Studies
In vitro experiments using human corneal epithelial cells, conjunctival cells, and macrophages provide mechanistic insight into how quercetin and gallic acid work at the cellular level. Eltanameli (2021) demonstrated that quercetin‑loaded chitosan nanoparticles significantly lowered IL‑6 expression and improved cell survival under hyperosmotic stress. Encapsulation boosted cellular uptake and reduced toxicity compared to free quercetin. Similarly, gallic acid showed strong antioxidant and anti‑inflammatory effects in corneal epithelial cells exposed to oxidative or osmotic stress. These findings confirm that nanoparticle delivery enhances intracellular availability and amplifies the therapeutic actions of both antioxidants.
Challenges in Clinical Translation
Despite promising preclinical evidence, several barriers remain before SLN‑based antioxidant therapies can reach clinical practice. The eye’s complex physiology—including tear turnover, blinking, and nasolacrimal drainage—makes it difficult to maintain therapeutic drug levels. Manufacturing challenges also exist: small variations in lipid composition or processing can alter particle size and stability, complicating scalability and reproducibility. Long‑term safety data are limited; while the lipids and surfactants used are generally considered safe, chronic exposure in humans requires thorough evaluation. Regulatory pathways for nanomedicines are still evolving, and proving bioequivalence to conventional formulations is difficult. Finally, patient comfort and acceptability must be addressed, as nanoparticle dispersions may cause temporary blurring or irritation if not carefully optimized.[23]
7. FUTURE PERSPECTIVES
The field of ophthalmic nanomedicine is advancing quickly, and solid lipid nanoparticles (SLNs) carrying antioxidants like quercetin and gallic acid are emerging as a strong foundation for next‑generation eye therapies. Yet, challenges remain in achieving long ocular retention, deep tissue penetration, and smooth clinical translation. Several innovative strategies—hybrid delivery systems, microneedle patches, evolving regulatory frameworks, and personalized nanomedicine—are poised to shape the future of this area.
Hybrid Systems: SLN‑Loaded Hydrogels
One promising approach is combining SLNs with hydrogels. Hydrogels made from Carbopol, hyaluronic acid, chitosan, or poloxamer‑based thermogels can form a viscoelastic layer on the eye’s surface, prolonging drug residence and reducing clearance by tears. Embedding SLNs within these gels creates a dual‑function system: the hydrogel ensures retention, while the SLNs provide controlled release and protect antioxidants from degradation. This strategy is especially useful for chronic conditions like dry eye disease, where sustained drug levels are critical. Thermoresponsive gels, which shift from liquid to gel upon contact with the eye, add comfort and ease of use for patients.
Microneedle Patches for Ocular Delivery
Microneedle technology is another exciting development. Patches applied to the sclera or periocular region can bypass the corneal barrier and deliver SLNs directly into deeper tissues such as the retina, choroid, or ciliary body—areas that are difficult to reach with eye drops. When loaded with quercetin or gallic acid, dissolving microneedles made from biocompatible polymers offer a painless, minimally invasive alternative to repeated intravitreal injections. Though still in early stages, this technology shows strong potential for treating posterior segment diseases driven by oxidative stress.
Regulatory Outlook
The regulatory pathway for ophthalmic nanomedicines remains complex. Agencies like the FDA and EMA require detailed data on nanoparticle size, stability, release kinetics, and long‑term safety. Reproducibility is a key concern, as small changes in lipid composition or processing can alter nanoparticle behavior. Robust toxicological studies are also essential, particularly for chronic use. As guidelines evolve, standardized testing protocols and clearer frameworks will be critical to accelerate clinical translation of SLN‑based antioxidant therapies.
Personalized Nanomedicine
The future of eye care is moving toward personalized nanomedicine, where formulations are tailored to each patient’s unique needs. Differences in tear composition, ocular surface inflammation, and disease severity can influence drug absorption and response. Customized SLN formulations—adjusted for lipid composition, drug ratios (quercetin vs. gallic acid), or release profiles—could optimize outcomes. Advances in 3D printing and microfluidic fabrication may enable patient‑specific dosing systems. Looking ahead, integrating SLNs with diagnostic biomarkers or biosensors could allow real‑time monitoring of oxidative stress or inflammation, paving the way for adaptive treatment strategies. [24,25]
CONCLUSION
Solid lipid nanoparticles (SLNs) are emerging as a powerful platform for delivering quercetin and gallic acid to the eye—two natural antioxidants with strong potential against diseases driven by oxidative stress. Their nanoscale size, biocompatible lipid matrix, and ability to encapsulate both hydrophobic and hydrophilic compounds allow for improved solubility, better corneal penetration, and sustained release. These features directly address the shortcomings of conventional eye drops, which are quickly cleared from the ocular surface and achieve very low bioavailability. By protecting quercetin and gallic acid from degradation, SLNs help ensure that effective concentrations reach target tissues.
Comparative studies show that while SLNs and nanostructured lipid carriers (NLCs) significantly improve permeability and stability, hot‑melt cast films can achieve even higher trans corneal flux thanks to prolonged surface contact and higher local drug concentrations. Films may therefore be particularly useful for anterior segment conditions like dry eye disease. However, they can cause discomfort and are less suitable for reaching posterior tissues, where SLNs and NLCs remain superior due to their deeper penetration and controlled release capabilities.
Encouraging preclinical evidence—from rabbit corneal permeability studies to cell‑based assays and mouse dry eye models—supports the therapeutic promise of these systems. Yet, clinical translation is still limited. Key challenges include demonstrating long‑term safety, achieving scalable and reproducible manufacturing, and navigating evolving regulatory frameworks for nanomedicines. Human ocular physiology also presents complexities that animal models cannot fully replicate, underscoring the need for carefully designed clinical trials.
In summary, SLNs provide a versatile and effective strategy for delivering quercetin and gallic acid to ocular tissues. Future research should prioritize optimizing dual‑loaded formulations, integrating SLNs into hybrid systems such as hydrogels, and conducting rigorous translational studies to bridge the gap between laboratory success and clinical application. [26,27]
REFERENCES


Dr. Satyam Chemate, Prashant Jare, Solid Lipid Nanoparticles (SLNS) For Ophthalmic Drug Delivery of Quercetin and Gallic Acid, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 1593-1607, https://doi.org/10.5281/zenodo.20567995
 10.5281/zenodo.20567995
10.5281/zenodo.20567995